X-rays of her wrists showed osteoarthritic changes to the first carpometacarpal (CMC) and trapezium-scaphoid joint without evidence of chondrocalcinosis. Ultrasound of her wrists showed prominent tenosynovial effusion, inhomogeneous synovium and abnormal power Doppler signals in the wrist joint.
Ultrasound can detect minimal amounts of intra-articular synovial fluid appearing as a compressible anechoic collection & can be used for needle guidance.
Aspiration of the effusion using ultrasound guidance revealed turbid synovial fluid with a leukocyte count of 5,200 per microliter with intracellular calcium pyrophosphate crystals. She had an incomplete response to colchicine, but did respond well to local ultrasound-guided injection to the tenosynovial sheath and radial carpal joint.
(click for larger image)
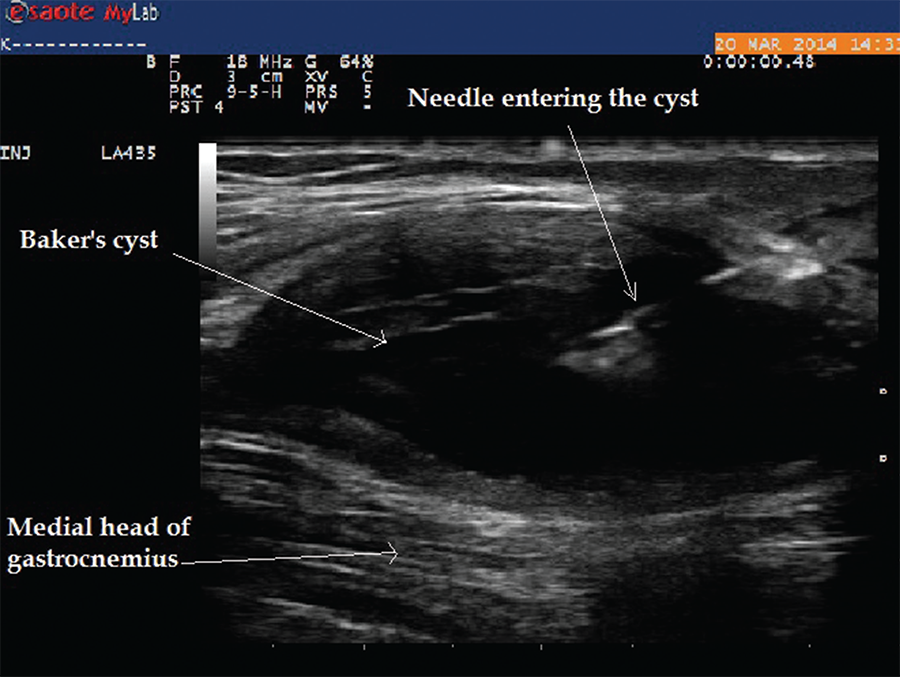
Image 9: The longitudinal view of Baker’s cyst. The medial gastrocnemius muscle is not seen on this view. The needle tip during aspiration using an in-plane technique can be visualized within the cyst.
Ultrasound findings of calcium pyrophosphate crystal deposition (CPPD) disease usually are seen within the hyaline cartilage and appear as hyperechoic spots that can be isolated, or form confluent spots that don’t generate an acoustic shadow.9 Similarly, calcium pyrophosphate dehydrate (CPP) deposition within fibro-cartilaginous structures, such as the meniscus, can appear as hyperechoic rounded or amorphous deposits. The medial meniscus of the knee is the most commonly affected cartilage among these patients.10
Presence of hyperechoic aggregates may be indicative of crystals; ultrasound-guided aspiration of these crystals can increase the sensitivity of diagnosis of the disease. Radiographs of multiple joints to prove the diagnosis can be cumbersome and exposes the patient to unnecessary radiation. The EULAR recommendations for CPP deposition suggest ultrasound is more sensitive and specific than X-rays for peripheral joints.11
Case 4
A 75-year-old female with a history of seronegative RA on low-dose prednisone, hydroxychloroquine and leflunomide presented to the rheumatology office with complaints of posterior knee pain and swelling, which had gradually worsened in the past month. She was compliant with her medications, and there was no recent change in her medications. Ultrasound of her knee demonstrated a large Baker’s cyst, and ultrasound-guided aspiration of the fluid demonstrated class I fluid. Typically, on a transverse view, boundaries of Baker’s cyst are formed by semimembranosus and semitendinosus of the medial aspect and medial gastrocnemius on the lateral aspect. Ultrasound allowed for diagnosis and therapeutic intervention during the same visit without the need to refer to radiology (see Images 9 and 10).