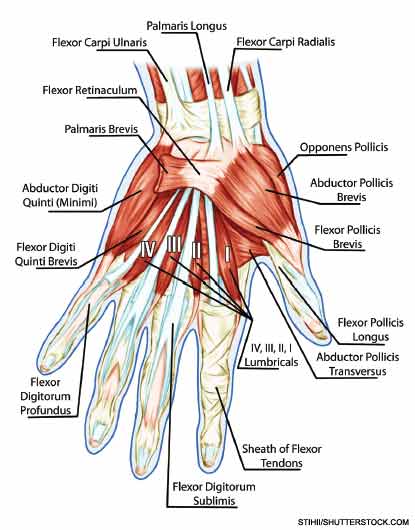
Figure 1: Anatomy of muscular system of the hand.
Pathomechanics of the Thumb CMC Joint
Ligamentous laxity and joint impingement: The movements at the thumb CMC joint explain the characteristic problems seen with thumb CMC joint OA. Laxity in the anterior oblique or “beak” ligament can predispose the thumb CMC joint to excessive pressure on the volar portion of the trapezium, particularly during lateral pinch activities such as holding a key.5 With beak ligament laxity, resisted pinching can lever the base of the metacarpal dorsally, resulting in volar compression and posterior translation of the base of the metacarpal. The dorsal/lateral subluxation of the metacarpal base produces the “shoulder sign,” a lateral prominence of the CMC joint, which has been associated with CMC OA (see Figure 2).


