Over the past decade and a half, cross-disciplinary research in immunology and bone biology has led to a revised picture for patients with rheumatoid arthritis. Pivotal work in the late 1990s to early 2000s demonstrated that, as in skeletal bone, osteoclasts were responsible for the destruction of articular bone—and that products of T cells and synovial fibroblasts, such as the receptor activator of ligand (RANKL), were of critical importance in inducing osteoclastogenesis in this setting.1-4 This knowledge, coupled with the rise of effective biologic agents to block inflammatory cytokines, has revolutionized what clinicians can offer to patients to arrest joint erosion.

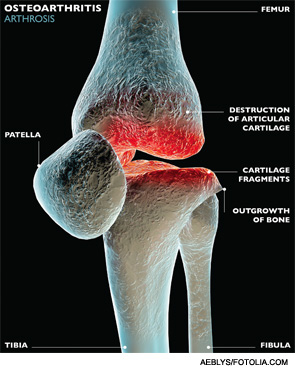
However, many questions remain to be answered for patients with rheumatoid arthritis and the more common joint disease, osteoarthritis. Why do some patients respond to anti-TNF agents while others do not? Does absence of inflammation always connote cessation of structural damage? Might there be an inflammatory component to development of osteoarthritis, despite the perception that it’s a degenerative process? Will an understanding of bone-immune system signaling lead to ways to induce bone repair?
Discoveries about the cross-talk between bone and the immune system in the burgeoning field of osteoimmunology may hold the key to these and other questions, and the development of more tools to address the disease process in other arthritides, according to researchers with whom we spoke.