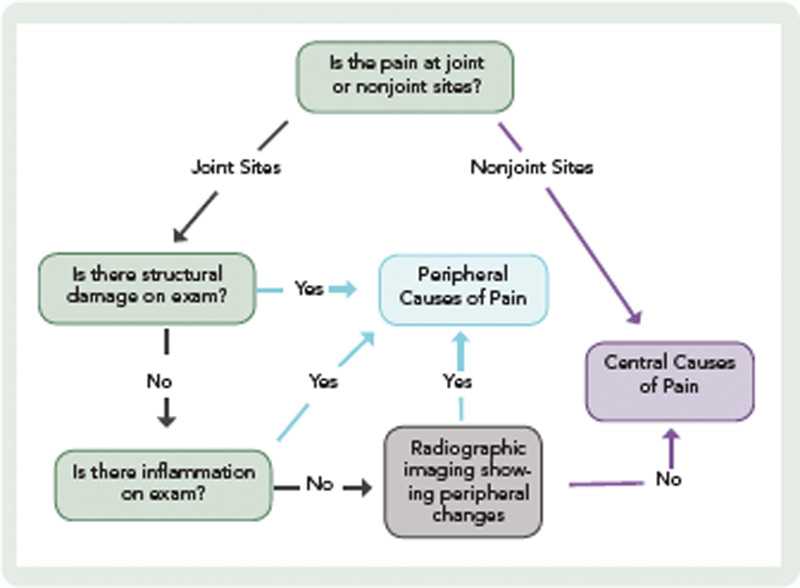
When assessing the location of pain, the main distinction is whether the pain is at joint or nonjoint sites. Pain at joint sites is more likely to be RA-related than pain at nonjoint sites. However, many patients may have pain at joint sites but no signs of inflammation or structural damage on physical examination. In these patients, it may be helpful to perform radiographic imaging via ultrasound or MRI to look for evidence of synovitis or erosions.
In the absence of radiographic findings, dysregulation of central pain processing mechanisms should be suspected, prompting the assessment of comorbid fibromyalgia. This assessment may be aided by the new ACR clinical and survey criteria for the diagnosis of fibromyalgia.12,13 These criteria do not require physical examination but are based on self-report measures that assess widespread pain and other symptoms (see Table 1).13 It is also important to ask the patient about fatigue, poor sleep, subjective cognitive problems, and/or psychiatric comorbidity (predominantly mood disturbance and anxiety). These symptoms are frequently present and can contribute, either individually or in concert, to the pain experience.