click for large version
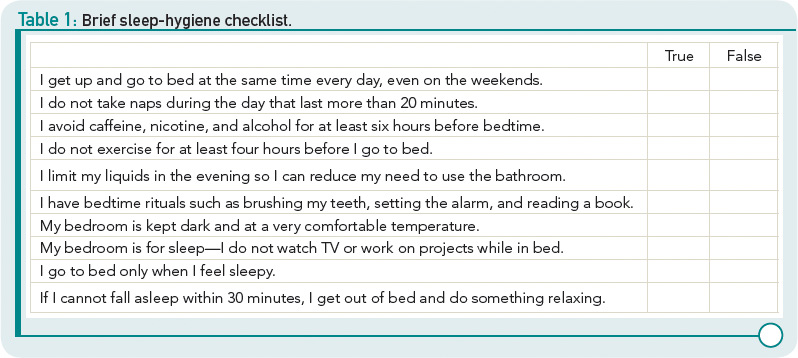
Table 1: Brief sleep-hygiene checklist.
Once you’ve identified the problem behaviors, encourage your patient to make changes and set concrete, but easily achievable, goals. It can be helpful to reassure patients that millions of people experience sleep disturbances and that the good news is that sleep problems can be frequently addressed with behavioral changes alone. If patients do not respond to simple sleep hygiene interventions, a referral to cognitive-behavioral therapy could be a good next step.


