In 1820, chemists Pierre Joseph Pelletier and Joseph Canentou isolated and purified quinine from Cinchona bark.3 From that time on, a standardized dose and purity for the drug was established. Eventually, the Dutch developed industrial-sized plantations of Cinchona in Java to supply the world antimalarial market.
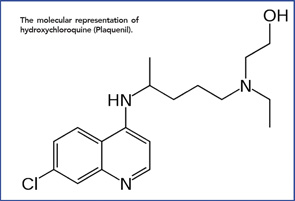
The molecular representation of hydroxychloroquine (Plaquenil).
When Japan overran Java in World War II, the world supply of natural quinine shrunk dramatically, just as Allied troops were pouring into the South Pacific. The solution? A synthetic version of quinine, quinacrine (Atabrine), became the drug of choice for the prevention of malaria.4 And the drug worked. As many as 3 million Allied soldiers ingested quinacrine prophylaxis daily for up to three years, with only rare side effects.5

