Better knowledge of rare diseases can improve diagnosis, reduce morbidity and streamline therapeutic decision-making. It can also help connect patients with the right treatments, clinical trials and supportive care, thus improving their outcomes.
Progress in rare disease research can also broaden the understanding of more common diseases, such as rheumatoid arthritis or vasculitis. By grouping people based on nearly identical clinical features of disease, it becomes easier to determine the disease’s genetic basis. In contrast to the complex genetics of common diseases, the smaller pool of genetic data associated with a rare disease can simplify the discovery process and help researchers home in on an illness-causing mutation.
As Dr. Miner says, “When we understand a particular disease pathway that’s affecting patients with an ultra-rare disease, it leads us to study those same pathways in common diseases and can guide us toward novel therapeutic targets for those more common rheumatic diseases.”
Connecting the Dots
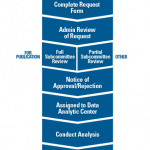
Increased access to data can further advance rare disease research. The internet has enabled patients and providers to more easily find information and connect around shared anomalies. More patients receive exome and genome sequences that can shed light on potential disease pathways. Providers are also increasing data sharing through registries and other means.
The ACR’s Rheumatology Informatics System for Effectiveness (RISE) registry collects data from electronic health records, including clinical note analysis. As a rheumatology-specific registry, RISE can provide data for research on rare rheumatic diseases. In the past five years, RISE data has been analyzed for four abstracts and two papers on rare rheumatic diseases, including ANCA-associated vasculitis and sarcoidosis.
Dr. Miner suggests that this is leading to the discovery of new patterns. “I often wonder how many of our patients with more common rheumatic diseases also have rare mutations—not just polymorphisms, but rare disease-causing variants—that haven’t been identified or characterized,” he says. As one example, mutations known to cause SAVI were recently found in some adults with ANCA-associated vasculitis, which is far more common.
“All clinicians see patients with syndromes presenting outside of the traditional, predictable ways,” Dr. Miner notes. “If there is only one RVCL patient in a practice, that patient could easily be misdiagnosed as having MS or SLE. When we don’t connect, we don’t learn of those uncommon cases in other practices. Increasing communication and data-sharing facilitates the proper diagnosis for our patients, helps us identify disease-causing mutations and is now leading to novel therapies that will likely benefit patients with common diseases.”