Conclusion: This process identified nine criteria that clinicians felt to be helpful or important in the diagnosis of JDM. A further process of refinement and validation is necessary to agree on an internationally acceptable, clinically usable set of diagnostic criteria.
Commentary
Evidence-based medicine requires studies; studies require accepted, well-standardized criteria. The Bohan and Peters criteria for dermatomyositis have served internist-rheumatologists well for more than 30 years. Pediatric rheumatologists have also used these criteria to advantage to make JDM diagnosis. However with advances in imaging technologies and the reluctance of pediatricians (and parents) to subject children to invasive procedures, many clinicians have drifted from the strict use of these criteria, primarily avoiding muscle biopsies and EMGs while retaining rash, proximal weakness, and elevated enzymes.
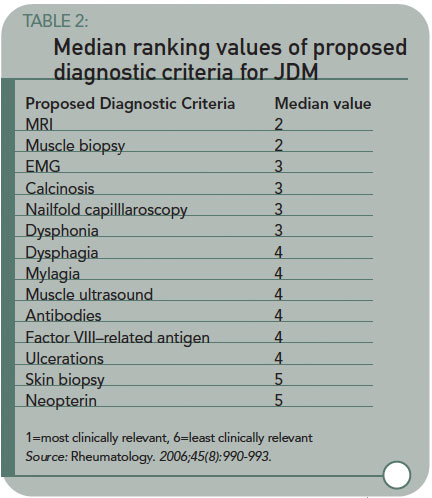
The authors have started the process of updating criteria for JDMS by a survey/consensus technique, identifying the diagnostic methods currently used, and found useful, by pediatric rheumatologists. Table 2 lists the diagnostic methods and the median usefulness rank for each. (See Table 2, above.) Magnetic resonance imaging of edema/inflammation in proximal muscles is taking the vote as a potential substitute for biopsy or EMGs. This also has its problems—cost, availability, and the fact that young children need to be sedated to get decent images.

