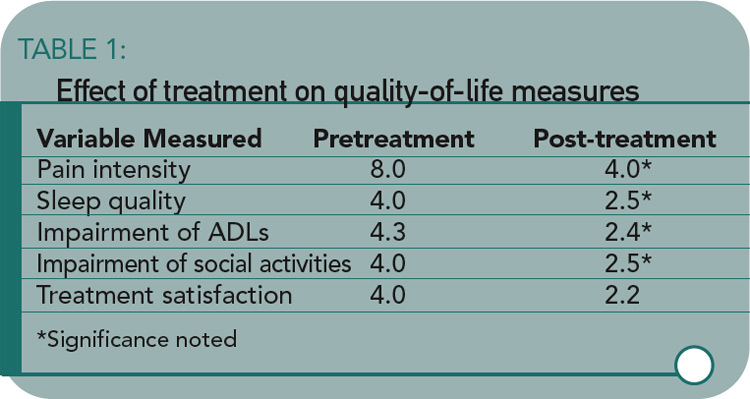
The study results showed significant improvement in pain intensity, sleep quality, activities, treatment satisfaction, and perceived general well-being. All variables other than pain intensity were measured on 5-point scales. (See Table 1)
There were a total of 75 adverse events in 39 (17%) of the patients. The most common were nausea (22%) and vomiting (16%). Few (1.3%) experienced constipation, which is generally acknowledged as an issue related to the use of opioids.2
About half of the sample (58%) agreed to be contacted at the end of six and 12 months to determine whether the initial study findings remained stable. The mean dose of fentanyl for this subgroup had increased from 28.8 µg/h at the end of 30 days to 49.1 µg/h at the end of 12 months. With this moderate increase in dose, all of the findings remained stable.
The study’s findings do indicate that transdermal fentanyl might be given consideration for pain management, as well as management of other symptoms (e.g., sleep quality and function) and of overall quality of life (e.g., coping with daily demands and feeling content). This is in keeping with the American Pain Society’s recommendation that “Opioids should be used for patients with OA and RA when other medications and nonpharmacologic interventions produce inadequate pain relief and the patient’s quality of life is affected by the pain.”2



