Conclusions:
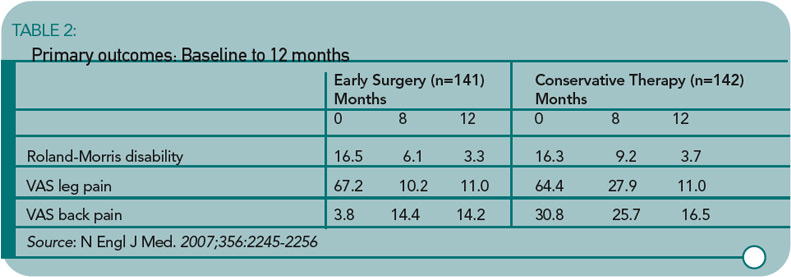
The one-year outcomes were similar for patients assigned to early surgery and those assigned to conservative treatment with eventual surgery if needed, but the rates of pain relief and of perceived recovery were faster for those assigned to early surgery.
Commentary
The patient with leg pain associated with a herniated intervertebral disc faces a number of treatment options. A herniated disc may heal spontaneously over a time period measured in months. Medical therapy including nonsteroidal anti-inflammatory drugs, analgesics, oral and/or injectable corticosteroids, and physical therapy can ease pain and decrease inflammation of damaged tissues during this time of disc resorption. Surgical intervention removes the offending piece of herniated nucleus pulposus with almost immediate resolution of leg pain. When patients are offered all of these options, the question frequently asked by those considering surgery is, What is the timeframe for a good outcome from an operation? The commonly quoted dictum is that surgery needs to be undertaken within 12 weeks of the onset of sciatica to have the best result.1 Peul and co-workers would disagree and state that the window of opportunity for a successful surgical outcome is six months or longer.

