The patient was diagnosed with ulnar nerve instability and dislocation of the ulnar nerve and MHTr. It was postulated that upon sudden elbow extension while vigorously throwing a baseball, ulnar nerve relocation occurred, with the ulnar nerve traumatically impacting either against the outside medial epicondyle and/or in the ulnar sulcus, producing severe pain.
Three days later the patient underwent anterior subcutaneous ulnar nerve transposition, in which the ulnar nerve was removed from the cubital tunnel. The MHTr was unaltered to avoid affecting his pitching velocity.
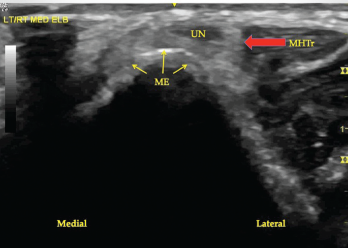
Figure 2. A transverse view of the ulnar groove in partial elbow flexion. Note the ulnar nerve and the medial head of the triceps muscle are both subluxing toward the apex of the medial epicondyle.
Three months later the patient resumed throwing a baseball and was soon able to painlessly pitch a complete season for a professional baseball team. He is now 14 months out from surgery and remains symptom free. His fastball remained greater than 90 mph and his earned run average was 2.32.
Causes of Medial Elbow Pain
In this age group, causes of medial elbow pain include medial epicondylitis, MCL injury with or without elbow instability, ulnar neuritis, snapping ulnar nerve, snapping triceps, olecranon osteophytes, olecranon stress fracture and flexor pronator strain.1
Ulnar neuritis may be caused by entrapment in different locations, but most commonly under Osborne’s ligament.1 Such entrapment is called cubital tunnel syndrome.2
Snapping ulnar nerve occurs in elbow flexion (between 70º and 90º) when the ulnar nerve dislocates over the apex of the medial epicondyle. This is typically painful and often accompanied by a palpable and audible snap.3,4 Neurologic symptoms from the snapping ulnar nerve are rarely reported, with the most common symptom being localized pain.3
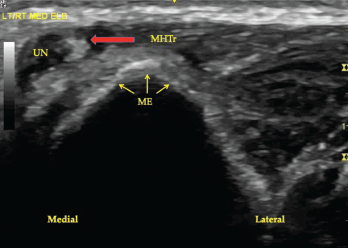
Figure 3. A transverse view of the ulnar groove in full elbow flexion. Note the ulnar nerve and the medial head of the triceps muscle have both dislocated over the apex of the medial epicondyle. Key: UN, ulnar nerve; MHTr, medial head of the triceps muscle; ME, medial epicondyle.