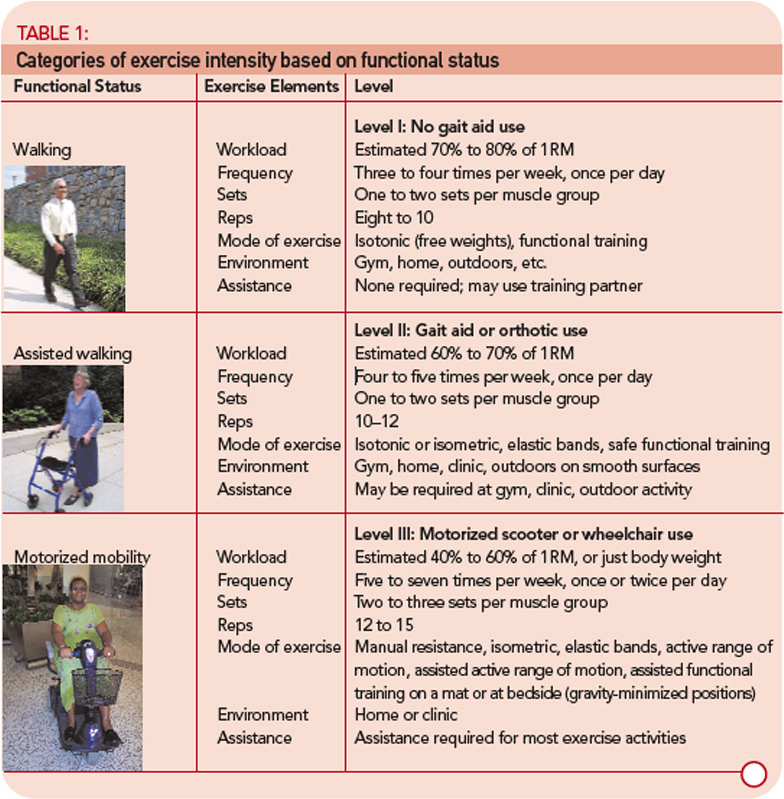
The initial exercise intensity may be informed by dynamometry tests performed in the clinic or simple estimates of the one-repetition maximum (1RM) using submaximal loads. (An online 1RM calculator can be found at www.exrx.net/Calculators/OneRepMax.html.) In my experience, many clinicians and patients are either unfamiliar or uncomfortable with identifying the 1RM. To address this concern, my colleagues and I have created exercise intensity categories based on the functional ability of the patient (see Table 1, p. 17). Using loads limited to the repetitions ascribed to each functional level will ensure that patients are engaging in strength training at the proper intensity to maintain safety and produce strength adaptations.
These intensity categories highlight the progressive resistance training paradox: high training intensity must be paired with low training volume, and low training intensity must be paired with high training volume. Strength training regimens at higher intensities require adequate recovery time for neuromuscular adaptations to occur, whereas strength training regimens at lower intensities require increased exercise volume to induce a training response and may constitute customary activity in the patients with severe muscle disease. Objective strength assessment is needed to identify optimal exercise intensity, and serial strength assessment is required to progress exercise intensity.
Recognize the Hidden Impairments
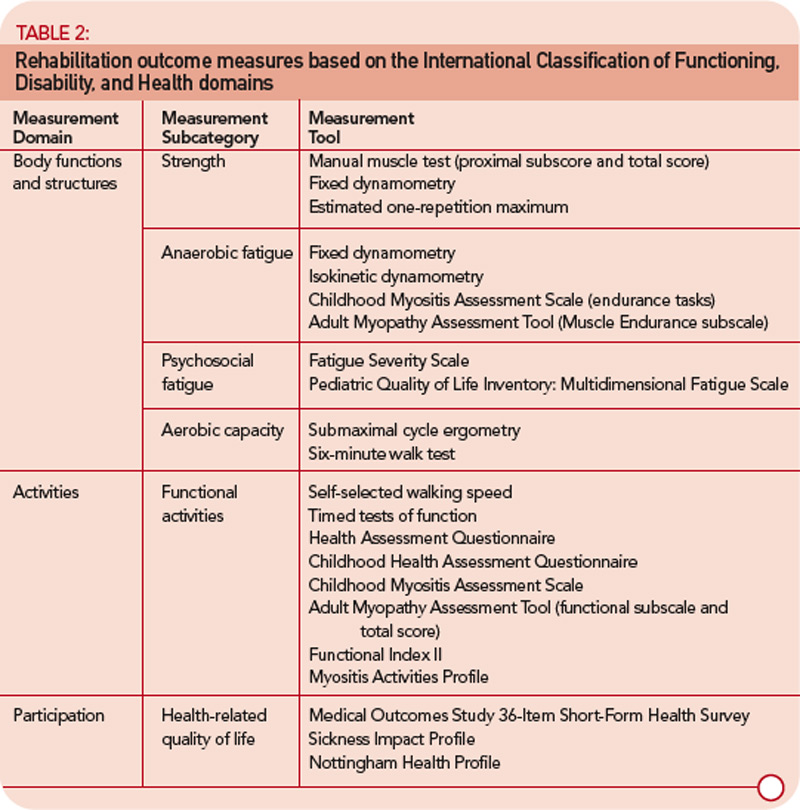
While muscle weakness is the most prominent impairment associated with myositis, it is important to not lose sight of the systemic, autoimmune etiology of this disease. Myositis is more than just a muscle disorder. The morbidity that results from myositis may involve the cardiovascular, pulmonary, gastrointestinal, and integumentary systems (recommended rehabilitation outcomes measures are listed in the Table 2, below left).2 Limitations in aerobic capacity may be due to capillary involvement in forms of inflammatory muscle disease such as dermatomyositis, or the result of inactivity secondary to muscle weakness.
The American College of Sports Medicine recommends aerobic activity at 40% to 85% of maximal oxygen consumption (VO2 max), 50% to 90% of maximal heart rate and 20 to 60 minutes in duration for three or more days per week (the range of values is designed to accommodate different levels of fitness). Muscle abnormalities may cause measures of aerobic performance such as the rate of oxygen consumption, heart rate, and respiration rate to underestimate the efforts expended by patients with myositis.5 Therefore, proxy measures of aerobic exercise intensity such as the Borg rating of perceived exertion (e.g., 13–14, or “somewhat hard” corresponds to 51% to 75% of VO2 max) or the Talk Test (i.e., difficulty speaking during aerobic exercise is related to the onset of anaerobic threshold) are patient-friendly tools that may be used to guide aerobic training regimens.5,6 Patients unable to exercise continuously for at least 20 to 30 minutes are encouraged to engage in multiple shorter periods of aerobic activity.


