
In our clinic, we have tried to address the shortcomings of the MMT in a couple of ways. Since summed MMT scores are more reliable than individual MMT grades, we report the percentage change in the MMT score in our patient notes and communications with physicians. At the 2005 ACR/ARHP Annual Scientific Meeting, my colleagues and I reported that the five weakest muscle groups in a cohort of 52 adult patients with polymyositis and dermatomyositis (based on MMT data collected by a single examiner) included the neck flexors, shoulder abductors, knee flexors, hip abductors, hip flexors, and hip extensors.4 We recommend use of the proximal muscle groups in summed MMT scores to capture the regions most affected by the disease and increase the responsiveness of the outcome measure. Our clinic has also elected to augment our strength assessments with dynamometry testing. But when should clinicians strive to use objective strength measurements, and what is the best dynamometry method to use?
Objective strength testing is indicated when a patient complains of strength deficits that you cannot detect on clinical examination, or for large muscle groups difficult to test using the MMT. Consequently, patients with large stature are natural candidates for strength assessment via dynamometry. Perhaps the most popular form of objective strength assessment is grip dynamometry. While grip dynamometry is relatively inexpensive, reliable, and easy to use, it cannot be used as a proxy measure of strength in patients with selective muscle weakness. This is certainly the case for patients with inclusion body myositis given the disproportionate involvement of their wrist flexors and knee extensors. Isokinetic dynamometry, while relatively expensive, offers superior stabilization during testing and provides a variety of testing modes. However, the time needed to conduct an isokinetic test precludes the testing of multiple muscle groups and it is difficult to position people with severe muscle weakness on the device.3
Handheld dynamometers provide more flexibility and less expense in comparison to isokinetic dynamometers. However, handheld dynamometers suffer from the same limitation as MMT: the outcome is dependent on the strength of the examiner. This type of device will exhibit high precision but low accuracy when used for large or strong muscle groups. The ideal objective strength-assessment device for both strong and weak patients is fixed dynamometry. Fixed dynamometers feature a plinth that allows for easy patient access and non-elastic straps attached to a frame to provide stabilization during testing (see Figure 1, below left). In our clinic, we record the clinical data from our dynamometry tests in absolute values, values scaled to body weight, and as a percentage of predicted force.
Progressive Resistance Training Paradox
The contributors to muscle weakness in adults with myositis include disease activity and damage, the effects of aging on muscle mass, and muscle atrophy secondary to inactivity. Exploratory clinical trials have shown that progressive resistance exercise is safe for people with acute and chronic myositis.1 Also, strength training has been successfully used to address the predictable decrease in muscle mass and power that is associated with sarcopenia. Successful exercise regimens depend on selecting the mode of treatment preferred by the patient and calculating the optimal exercise intensity. Multiple factors contribute to exercise intensity, but the most commonly cited element is load (i.e., the amount of weight lifted). Typical errors in the exercise prescription for strength training include using initial intensity levels that are too high or selecting low levels of intensity without a progression scheme.
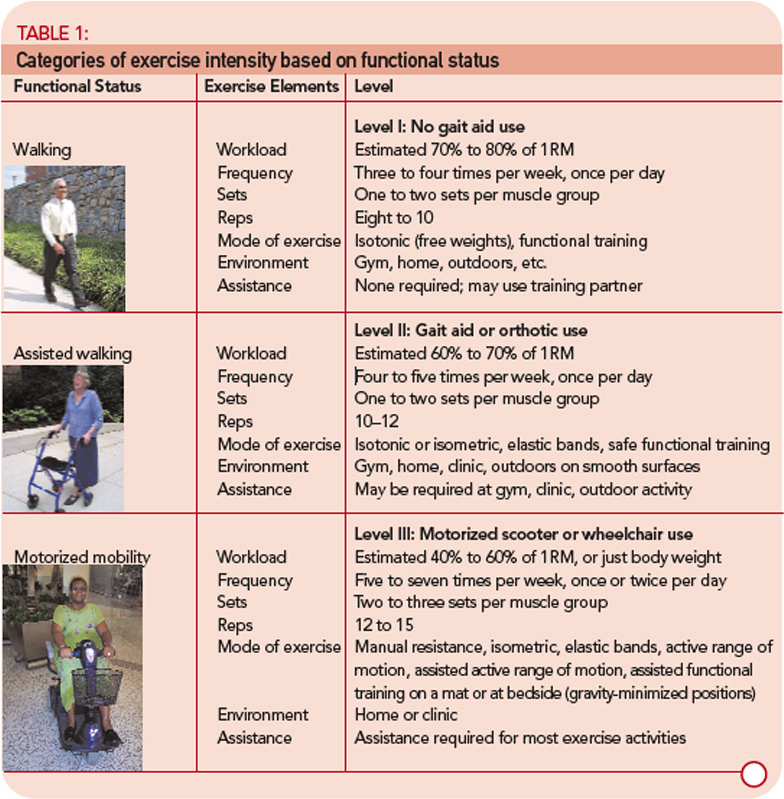
The initial exercise intensity may be informed by dynamometry tests performed in the clinic or simple estimates of the one-repetition maximum (1RM) using submaximal loads. (An online 1RM calculator can be found at www.exrx.net/Calculators/OneRepMax.html.) In my experience, many clinicians and patients are either unfamiliar or uncomfortable with identifying the 1RM. To address this concern, my colleagues and I have created exercise intensity categories based on the functional ability of the patient (see Table 1, p. 17). Using loads limited to the repetitions ascribed to each functional level will ensure that patients are engaging in strength training at the proper intensity to maintain safety and produce strength adaptations.
These intensity categories highlight the progressive resistance training paradox: high training intensity must be paired with low training volume, and low training intensity must be paired with high training volume. Strength training regimens at higher intensities require adequate recovery time for neuromuscular adaptations to occur, whereas strength training regimens at lower intensities require increased exercise volume to induce a training response and may constitute customary activity in the patients with severe muscle disease. Objective strength assessment is needed to identify optimal exercise intensity, and serial strength assessment is required to progress exercise intensity.
Recognize the Hidden Impairments
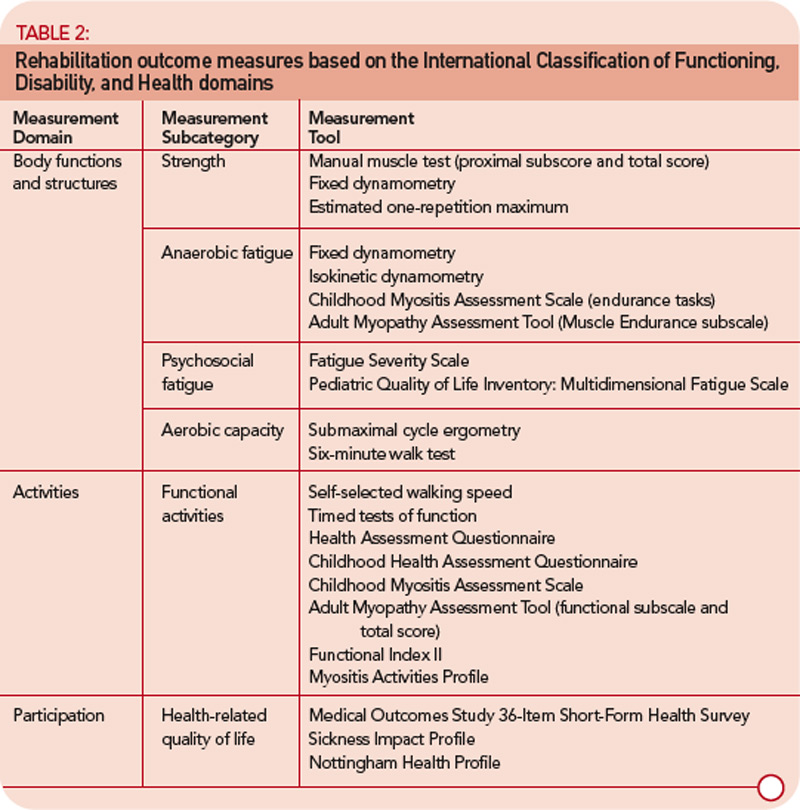
While muscle weakness is the most prominent impairment associated with myositis, it is important to not lose sight of the systemic, autoimmune etiology of this disease. Myositis is more than just a muscle disorder. The morbidity that results from myositis may involve the cardiovascular, pulmonary, gastrointestinal, and integumentary systems (recommended rehabilitation outcomes measures are listed in the Table 2, below left).2 Limitations in aerobic capacity may be due to capillary involvement in forms of inflammatory muscle disease such as dermatomyositis, or the result of inactivity secondary to muscle weakness.
The American College of Sports Medicine recommends aerobic activity at 40% to 85% of maximal oxygen consumption (VO2 max), 50% to 90% of maximal heart rate and 20 to 60 minutes in duration for three or more days per week (the range of values is designed to accommodate different levels of fitness). Muscle abnormalities may cause measures of aerobic performance such as the rate of oxygen consumption, heart rate, and respiration rate to underestimate the efforts expended by patients with myositis.5 Therefore, proxy measures of aerobic exercise intensity such as the Borg rating of perceived exertion (e.g., 13–14, or “somewhat hard” corresponds to 51% to 75% of VO2 max) or the Talk Test (i.e., difficulty speaking during aerobic exercise is related to the onset of anaerobic threshold) are patient-friendly tools that may be used to guide aerobic training regimens.5,6 Patients unable to exercise continuously for at least 20 to 30 minutes are encouraged to engage in multiple shorter periods of aerobic activity.
The secondary balance impairment that results from muscle weakness poses an additional barrier to aerobic fitness. Physical therapists should review aerobic training alternatives with their patients such as the recumbent stationary bicycle and upper-extremity ergometry. The initial session of upper-extremity ergometry should be closely monitored since it is about 25% less efficient than lower-extremity ergometry and has higher oxygen demands. Understanding the methods to monitor aerobic intensity and using creative approaches to exercise safely will allow the patient and physical therapist to craft an effective training program. By using serial strength assessments to monitor chronic disease, determining the appropriate progressive resistance exercise intensity, and being aware of the impairments of myositis that extend beyond weakness, physical therapists can play a valuable role in the clinical management of inflammatory muscle disease.
Dr. Harris-Love is assistant professor of physical therapy at the George Washington University School of Medicine and Health Sciences in Washington, DC and a visiting researcher in the Environmental Autoimmunity Group at the National Institute of Environmental Health Sciences in Bethesda, Md.
References
- Harris-Love MO. Physical activity and disablement in the idiopathic inflammatory myopathies. Curr Opin Rheumatol. 2003;15(6):679-690.
- Miller FW, Rider LG, Chung YL, et al. Proposed preliminary core set measures for disease outcome assessment in adult and juvenile idiopathic inflammatory myopathies. Rheumatology. 2001;40(11):1262-1273.
- Rider LG, Giannini EH, Harris-Love M, et al. Defining clinical improvement in adult and juvenile myositis. J Rheumatol. 2003;30(3):603-617.
- Moini B, Harris-Love MO, Pokrovnichka A, Pahlajani N, Barham B, Plotz P. Muscle weakness in myositis: where to look? Arthritis Rheum. 2005;52(9):S434-S434.
- Hicks JE, Drinkard B, Sunmers RM, Rider LG. Decreased aerobic capacity in children with juvenile dermatomyositis. Arthritis Rheum. 2002;47(2):118-123.
- Persinger R, Foster C, Gibson M, Fater DC, Porcari JP. Consistency of the talk test for exercise prescription. Med Sci Sports Exerc. 2004;36(9):1632-1636.


