 Defining remission in rheumatoid arthritis (RA) is more important than ever now that we have therapies that put remission within the reach of our patients. David T. Felson, MD, MPH, professor of medicine, Division of Rheumatology, Boston University School of Medicine, and lead author on the 2011 ACR/EULAR RA Remission Criteria and a recent Arthritis & Rheumatology editorial that put forth these definitions, offers insight into what remission means for practicing rheumatologists.
Defining remission in rheumatoid arthritis (RA) is more important than ever now that we have therapies that put remission within the reach of our patients. David T. Felson, MD, MPH, professor of medicine, Division of Rheumatology, Boston University School of Medicine, and lead author on the 2011 ACR/EULAR RA Remission Criteria and a recent Arthritis & Rheumatology editorial that put forth these definitions, offers insight into what remission means for practicing rheumatologists.
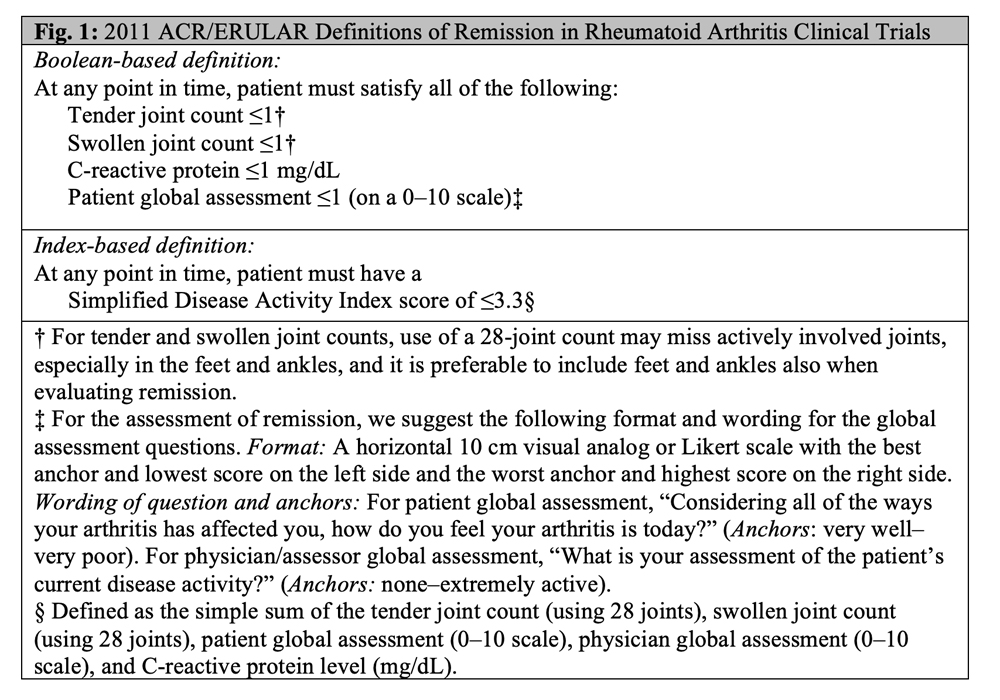
2011 ACR/EULAR Definition of Remission in RA
In 2011, the ACR/EULAR published two data-driven consensus definitions of remission in RA that best predicted “absence of X-ray damage progression and good functional outcomes in the future” (see Figure 1, right).1 The first is a Booleanbased definition that requires a patient to satisfy all of the following: both a tender and a swollen joint count of less than or equal to 1, a C-reactive protein (CRP) level of less than or equal to 1 mg/dL, and a patient global assessment (PGA) of arthritis activity of less than or equal to 1 on a 0–10 scale. The second is a Simplified Disease Activity Index (SDAI) score of less than or equal to 3.3. The SDAI is a sum of the tender and swollen joint counts, CRP level, PGA and provider global assessment of arthritis activity.2
Since publication of the provisional criteria, three main concerns have arisen: the ongoing use of the DAS28 to define remission in clinical trials, the use of CRP as part of remission definitions and the appropriateness of including PGA in remission definitions. Felson et al. addressed each concern in an editorial in January.3
DAS28
Despite a lack of endorsement in the 2011 ACR/EULAR recommendation for use as an RA remission definition, the DAS28 continues to be used in clinical trials. The DAS28 comprises the tender joint count, swollen joint count, PGA and CRP level. However, not all components are equally weighted.

Dr. Felson
“I co-chaired the ACR/EULAR Definition of Remission Committee in 2011,” says Dr. Felson. “We wanted to include the DAS28 because it’s so popular, but we couldn’t find a threshold—that is, even a very low DAS28 score—that worked because the formula is basically a weighted tender joint count. If your tender joint count is low, you can reach DAS28 remission … even with several swollen joints or an elevated PGA. It doesn’t matter what else is going on.”
“Practicing rheumatology providers shouldn’t be reassured by DAS28 remission in clinical trials,” he continues. “Publications often highlight DAS28 remission. Some of these patients have no disease activity … but often that’s genuinely not the case. Unfortunately, [because] DAS28 yields remission rates far higher than definitions supported by the ACR/EULAR, treatments can appear more effective than they really are in RA trials focusing on remission report only DAS28 remission.”
CRP Levels
The use of CRP levels as part of remission definitions is also imperfect. CRP is the second-most heavily weighted item in the DAS28 formula, but several biologic agents directly reduce CRP regardless of patient status (e.g., interleukin 6 and Janus kinase inhibitors) and several don’t reduce CRP even if the patient improves (e.g., rituximab and abatacept).4
“Remission definitions that are dependent on acute phase reactants are not serving us well in the new world [in which] some therapies directly target them,” says Dr. Felson. “That means we get measures of disease activity that aren’t consistent across treatments in clinical trials, which makes it hard to compare efficacy.
“The CRP level is indeed included in the 2011 ACR/EULAR recommended Boolean-based and SDAI definitions for RA remission, but it is not weighted nearly as much as in the DAS28,” he clarifies. “Further, there are alternate ACR/EULAR recommended measures of remission that don’t include CRP, including the Clinical Disease Activity Index (CDAI) and the three-measure Boolean definition [i.e., tender joint count, swollen joint count and PGA].”
PGA
The appropriateness of including the PGA in remission criteria has also been questioned because the PGA is a subjective measure. We can all agree a patient’s assessment of their arthritis activity may be influenced by more than just joint pain and swelling. In addition to fatigue, patients may have a low 28-joint count yet a high PGA score because they have pain in joints the 28-joint count did not include, such as the feet, ankles, hips or neck.
However, Dr. Felson points out that this patient-reported outcome remains a powerful predictor of overall function as measured by the Health Assessment Questionnaire (HAQ), and high PGAs identify those patients whose physical function is worsening.5 Further, the PGA is a sensitive outcome measure that may shed light on disease activity driven by systemic inflammation.6
“We all ask patients, ‘How are you doing from an arthritis perspective?’ in one way or another,” says Dr. Felson. “This is our PGA. If patients say their arthritis is active, they are often right even though a cursory joint exam may miss the source of disease activity. This report of active disease should trigger an evaluation to help determine whether treatment should be changed. On the one hand, they could have pain or fatigue that is unrelated to active RA. Just as likely, though, is that the patient could be fatigued and exhausted due to active RA. Or perhaps there is involvement somewhere beyond what the 28-joint count examined.”
When it comes to patients who always report a PGA of 10 out of 10 no matter what, Dr. Felson offers the following advice: “A high PGA should prompt you to look closer. Then, use your clinical judgment to determine if the score is being driven by RA itself or something else, like fibromyalgia.”
Editors’ Note
Thanks to this editorial, the five journals of the ACR and EULAR jointly agreed to “enforce the use of the products obtained in the course of joint ACR/EULAR or EULAR/ACR activities in all respective papers.”3 For RA, this means the use of ACR/EULAR remission definitions and classification criteria will need to be addressed for manuscripts to be published in these journals. The same will apply for other diseases.
The editors explain that “maintaining uniformity across major publications … not only allows for more appropriate comparison across analyses, but also enhances readers’ ability to interpret results.”3
Conclusion
Defining remission in RA is of utmost importance in a day and age in which remission is within reach. The DAS28 should not be used to define remission because, by this metric, many patients still have swollen joints, and its dependence on CRP values compromises validity with some newer therapies. Although the PGA is subjective, defining remission without including any kind of patient-reported outcome would be remiss.
Samantha C. Shapiro, MD, is an academic rheumatologist and an affiliate faculty member of the Dell Medical School at the University of Texas at Austin. She received her training in internal medicine and rheumatology at Johns Hopkins University, Baltimore. She is also a member of the ACR Insurance Subcommittee.
References
- Felson DT, Smolen JS, Wells G, et al. American College of Rheumatology/European League Against Rheumatism provisional definition of remission in rheumatoid arthritis for clinical trials. Arthritis Rheum. 2011 Mar;63(3):573–586.
- Smolen JS, Breedveld FC, Schiff MH, et al. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology (Oxford). 2003 Feb;42(2):244–257.
- Felson DT, Lacaille D, LaValley MP, et al. Reexamining remission definitions in rheumatoid arthritis: Considering the twenty-eight–joint disease activity score, C-reactive protein level and patient global assessment. Arthritis Rheumatol. 2022 Jan;74(1):5–9.
- Aletaha D, Nell VPK, Stamm T, et al. Acute phase reactants add little to composite disease activity indices for rheumatoid arthritis: Validation of a clinical activity score. Arthritis Res Ther. 2005;7(4):R796–806.
- Ferreira RJO, Welsing PMJ, Jacobs JWG, et al. Revisiting the use of remission criteria for rheumatoid arthritis by excluding patient global assessment: An individual meta-analysis of 5792 patients. Ann Rheum Dis. 2020 Oct 6;annrheumdis-2020-217171.
- Felson DT, Anderson JJ, Boers M, et al. The American college of rheumatology preliminary core set of disease activity measures for rheumatoid arthritis clinical trials. Arthritis Rheum. 1993 Jun;36(6):729–740.
