Temporal arteritis was first described by Sir Jonathan Hutchinson in 1890 in an elderly retired gentleman’s servant who developed red, painful streaks on his temples and was found to have bilaterally swollen temporal arteries with feeble pulses.1 Sir Hutchinson disputed the suggestion that the red streaks were caused by the man’s hat and, instead, called his observation, albeit without histology, “an unquestionable example of an arteritis, which spread along the affected vessels, causing swelling of the external coats and adjacent cellular tissue which resulted very quickly in occlusion of the vessels.”
Temporal arteritis is a form of the medium to large vessel arteritis named giant cell arteritis.
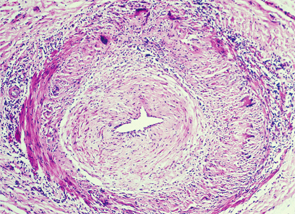
Pathology
More than a century has passed since this initial observation, but the sequence of events precipitating the arteritis remains unclear.

