click for large version
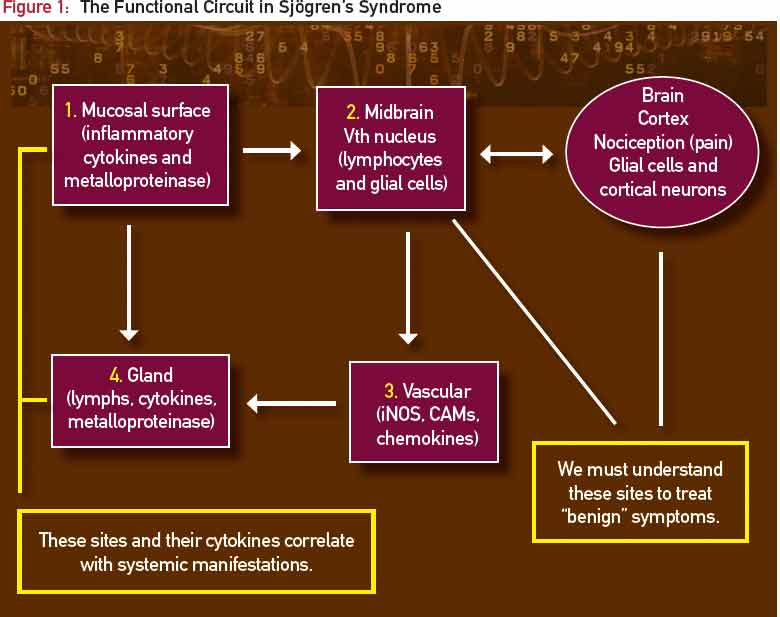
Figure 1: The Functional Circuit in Sjögren’s Syndrome
click for large version
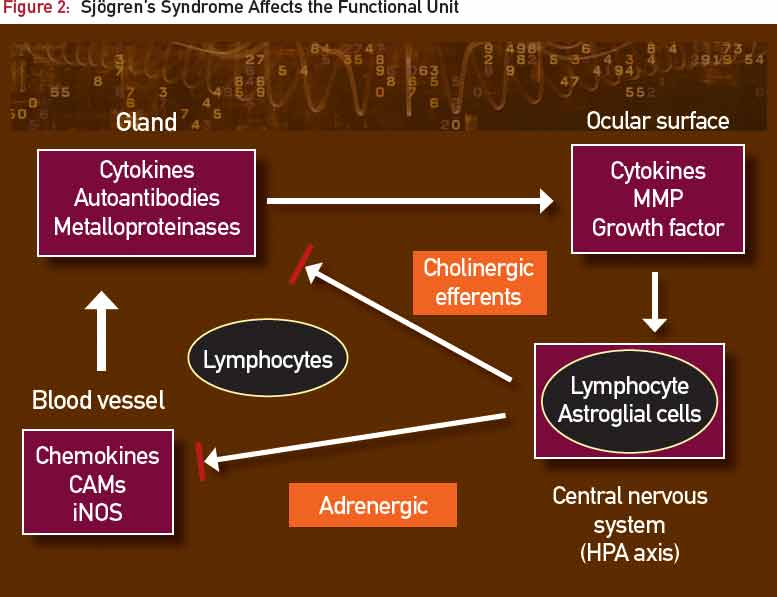
Figure 2: Sjögren’s Syndrome Affects the Functional Unit
click for large version
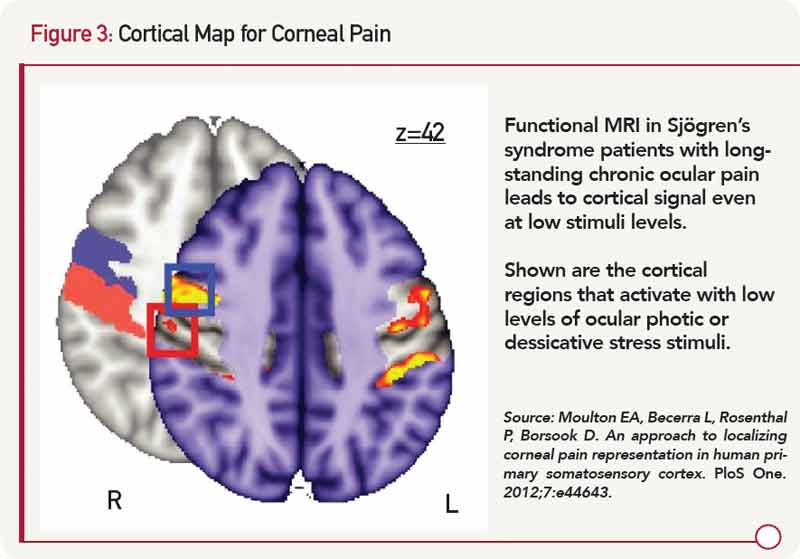
Figure 3: Cortical Map for Corneal Pain
Phantom Pain and Ocular Pain in SS
As noted earlier, ocular symptoms in patients with SS are out of proportion with objective observations of the ocular surface, largely due to the mysterious perception of “phantom pain.”


