click for large version
Figure 1: Clinical Conceptualization of the Natural History of axSpA: An Emerging Model
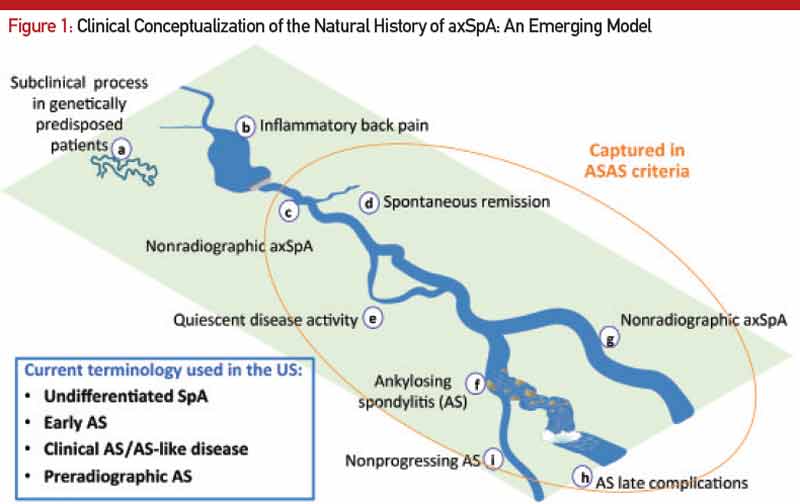
Here, the course of axial SpA is compared to the course of a river. A) Some people may be genetically predisposed to develop axial SpA but may never develop any clinical manifestations of the condition or may have a subclinical disease. B) According to the recent NHANES study (2009–2010), inflammatory back pain is found in 6% of U.S. population, but only a small percentage of those will develop C) nonradiographic axial SpA (nr-axSpA). D) A small percentage of these people may have a spontaneous remission, and E) some may have a quiescent disease course. F) Studies have shown that up to 12% of nr-axSpA patients develop ankylosing spondyloarthritis (radiographic sacroiliitis) in two years; whereas, others may continue as G) nr-axSpA. Not all ankylosing spondylitis patients have a progressive course, either. Some progress to develop long-term complications H), and others may have a relatively benign but chronic course I). Adapted from van Vollenhoven RF. Nat Rev Rheumatol. 2011 Apr;7(4):205–215.
Here, the course of axial SpA is compared to the course of a river. A) Some people may be genetically predisposed to develop axial SpA but may never develop any clinical manifestations of the condition or may have a subclinical disease. B) According to the recent NHANES study (2009–2010), inflammatory back pain is found in 6% of U.S. population, but only a small percentage of those will develop C) nonradiographic axial SpA (nr-axSpA). D) A small percentage of these people may have a spontaneous remission, and E) some may have a quiescent disease course. F) Studies have shown that up to 12% of nr-axSpA patients develop ankylosing spondyloarthritis (radiographic sacroiliitis) in two years; whereas, others may continue as G) nr-axSpA. Not all ankylosing spondylitis patients have a progressive course, either. Some progress to develop long-term complications H), and others may have a relatively benign but chronic course I). Adapted from van Vollenhoven RF. Nat Rev Rheumatol. 2011 Apr;7(4):205–215.
MRI of the sacroiliac (SI) joints has emerged as the imaging investigation of choice for patients with suspected axSpA who do not have X-ray evidence of sacroiliitis. On T2-weighted fat-suppressed sequences (called STIR sequences) of the MRI, active inflammatory lesions of osteitis are seen as bone marrow edema (BME). MRI can also detect other lesions, such as synovitis, enthesitis and capsulitis, associated with SpA. Among these, the clear presence of a single osteitis lesion on two consecutive slices or two osteitis lesions on a single MRI slice is considered essential for defining active sacroiliitis.8 Structural damage lesions, such as sclerosis, erosions, fat deposition and ankylosis can also be detected by MRI on T1-weighted images.9



