click for large version
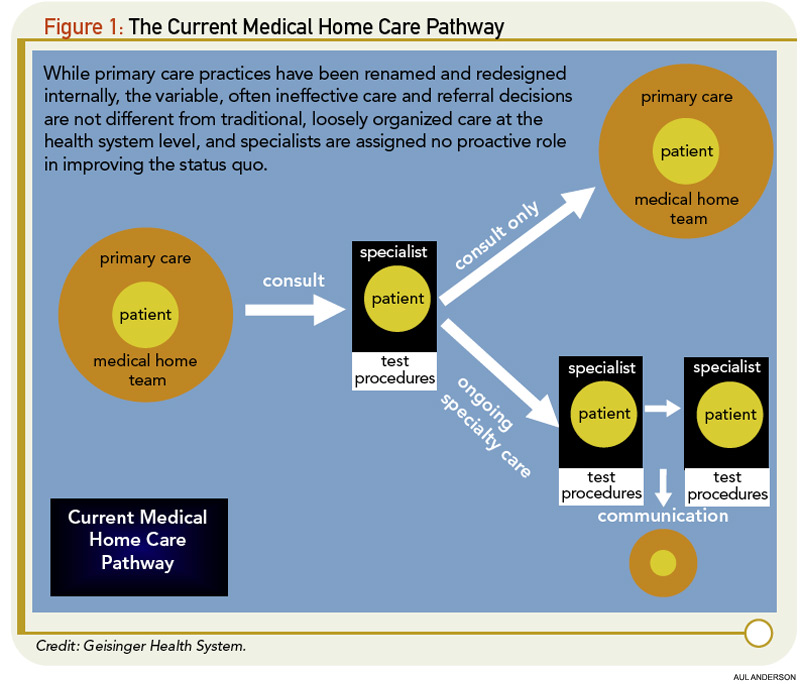
Figure 1: The Current Medical Home Care Pathway
The initial experiences, including our own, with the Medical Home have been mixed for managing musculoskeletal diseases. Optimal osteoporosis care has not been supported in systems adopting the Medical Home. At Kaiser Permanente, a highly successful system-based program has been developed instead of using the Medical Home for this purpose.23 Results of a recent study indicate that implementing a Medical Home within the University of Wisconsin Medical Foundation (UWMF) has actually interfered with osteoporosis care that previously was provided effectively and efficiently through a system-based coordination program.24


