In the past, when treatment options were limited, the natural history of RA involved severe outcomes in both men and women over the course of disease of five to 20 years.13 Severe long-term outcomes of RA were reported equally in women and men in terms of clinical disease activity, structural damage, and deformities.14-19 At present, the health status of RA patients is significantly better compared with that observed in previous decades, according to a variety of measures including disease activity, function and structural outcomes, work disability, and mortality rates.20-30 Importantly, these measures do not show a sex preference. Nonetheless, as in the general population, men with RA have considerably higher mortality rates than women.31
Gathering Data on Sex Differences and RA
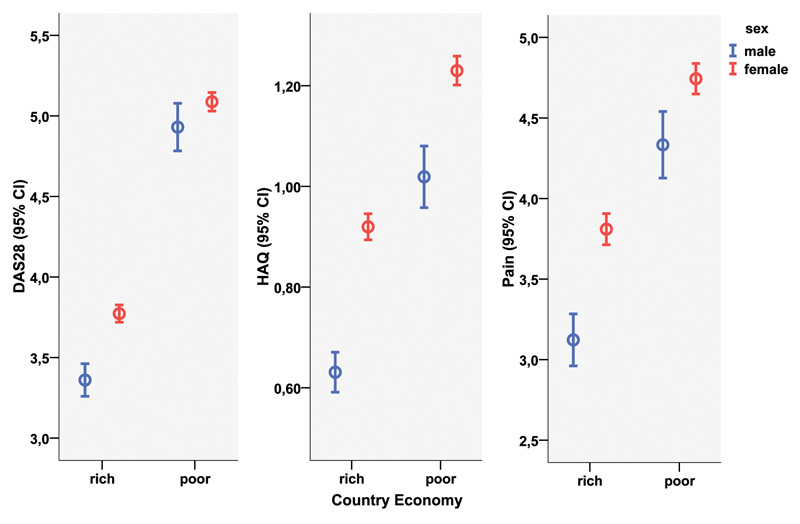
What, therefore, accounts for the sudden change in the view that RA is worse in women than in men? With this question in mind, my colleagues and I sought to analyze in our research the possible influence of sex differences on the clinical status and course of RA in a large, multinational, clinical RA database.32
