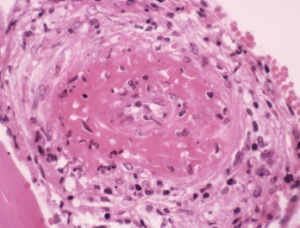
Light micrograph of a section through a human artery, showing a large thrombus (blood clot, center) due to cryoglobulinemia.
CNRI / Science Source
A study that focused on the detection and immunological characteristics of cryoglobulins provides insights for rheumatologists and other rheumatology providers, as well as lab professionals.
Co-researchers Marie N. Kolopp-Sarda, PharmD, PhD, and Pierre Miossec, MD, PhD, Clinical Immunology Unit, Department of Immunology and Rheumatology, University of Lyon, France, included in their retrospective study, published in Arthritis & Rheumatology, a large cohort of 13,439 patients who were tested for cryoglobulins—immunoglobulins (Ig) that precipitate in cold temperatures—from January 2010 to December 2016 in Lyon.1