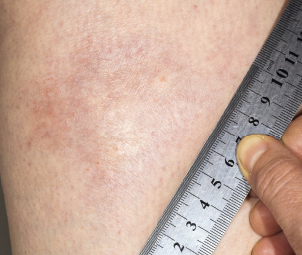
A morphea plaque on the leg.
Dr Harout Tanielian / Science Source
In September 2018, the U.S. Food & Drug Administration (FDA) granted fast-track status to FCX‑013, a gene therapy product developed to treat moderate to severe localized scleroderma (morphea). Previously, the treatment received an orphan drug designation for localized scleroderma, as well as a rare pediatric disease designation. Phase 1 and 2 studies will assess safety and suggest whether FCX-013 holds promise for this damaging disease, which currently lacks FDA-approved treatments.
Systemic Sclerosis & Localized Scleroderma
The sclerotic disease, scleroderma, can be classified as two distinct autoimmune syndromes: systemic sclerosis and localized scleroderma. Although the latter is thought to only rarely progress to the former, the two share overlapping findings in histology, cell biology and pathophysiology. Systemic sclerosis is characterized by cutaneous sclerosis and deep visceral involvement, whereas localized scleroderma primarily causes skin symptoms. However, localized scleroderma encompasses a spectrum of different skin depths and patterns of lesions. In some subtypes, localized scleroderma may also affect nearby tissues, such as fat, fascia, muscle and bone.1,2


