BALTIMORE—There’s an increasing interdisciplinary interest in connective tissue disease-associated interstitial lung disease, according to Colorado-based rheumatologist Aryeh Fischer, MD, the lead author of a special article about an international summit of experts on the topic. The article was co-published in the February 2019 issues of the ACR’s journal Arthritis & Rheumatology, as well as the Association of Physicians of Great Britain and Ireland’s QJM: An International Journal of Medicine.1
Aryeh Fischer, MD
“There’s a growing appreciation for unmet needs, challenges and opportunities in this domain,” Dr. Fischer says.
- Clinical;
- Biomarkers;
- Diagnostic imaging and histopathology;
- Treatment and clinical trials design and outcome measures; and
- Translational research.
The Complexities of ILD
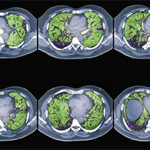
ILD, an overarching term for a group of lung disorders characterized by scarring and/or inflammation in the lung parenchyma, is a common manifestation of CTD and often results in significant morbidity and mortality. Although all CTD patients can develop ILD, those with systemic sclerosis, polymyositis/dermatomyositis and rheumatoid arthritis (RA) are at particularly high risk.
A patient with CTD can develop ILD at any time, but ILD may also present as the first clinically apparent feature of an otherwise undiagnosed CTD. Diagnosing CTD-associated ILD as early as possible can help determine treatment decisions, assist with surveillance for other autoimmune clinical features, as well as help ascertain a patient’s prognosis. And although ILD can be devastating and progressive, as in the case of idiopathic pulmonary fibrosis, some CTD patients develop mild forms of ILD that are not progressive in nature.
Collaboration
The summit underscored that collaboration among rheumatologists and pulmonologists is key to accurately diagnosing, evaluating and treating patients with these diseases.

Attendees of the summit discussed key clinical and research aspects of the complex intersection between connective tissue diseases and ILD.
“There is a growing appreciation that this is not a rheumatology problem or a pulmonology problem in isolation,” says Dr. Fischer. “Essentially, this [care] is reaching across the aisle with respect to interdisciplinary engagement. Pulmonologists need to engage rheumatologists. Rheumatologists need to engage pulmonologists, and we need to work together to provide better education.”
Rheumatology fellows, Dr. Fischer says, need pulmonary training just as pulmonary fellows should have rheumatology training. “It starts with how we speak to our fellows, with how we speak to our colleagues, with how we train them,” he says. “Patients shouldn’t be finding out 20 years into having RA that it can affect the lungs. The lungs are involved in about one-third to half of RA patients and many patients have no idea.”
Although some rheumatologists or select centers have begun screening for lung disease in CTD patients, the level of expertise in this area is varied and rheumatologists lack clear guidelines for such assessments. In Dr. Fischer’s opinion, any RA patient who hasn’t been assessed for lung involvement as part of their evaluation should ask their rheumatologist to consider such testing.
“It’s part of the disease. The eyes are affected in a subset of patients. It’s not an arthritic condition in isolation. It’s a systemic autoimmune disease,” he says, adding that in other complex autoimmune diseases, such as lupus, the lungs are among favorite targets of the disease.
Challenges to Diagnosis
Although a multidisciplinary approach to diagnosing and treating these diseases is ideal, practical limitations remain and, often, effective collaboration between the two specialties is lacking.
Current approaches to screening CTD patients for ILD, or those who are at the highest risk for developing it, are insufficient, according to the report. The ideal approaches require identifying ILD in its earliest stages in combination with identifying patients who are at the greatest risk for disease progression and a decline of function.
Currently, diagnosing patients with CTD-associated ILD includes integration of the physical examination, history, testing of pulmonary function, lung imaging and histopathology studies. No validated biomarkers for the disease exist, which are important due to the heterogeneity of ILD. The report says biomarkers can become important tools in clinical practice, but specific measures should be accurate, accessible and reproducible.
Other unmet needs include accurate diagnostic imaging, an integration of histopathology, clinical trials and better treatment options. Example: No risk/benefit analysis has been conducted for the invasive procedure of undergoing a lung biopsy in these patients. However, CTD patients’ lung biopsies often reveal features of an autoimmune disease. These histopathologies are the gold standard in identifying fibrosis, and they may assist with determining a prognosis.
Although broad immunosuppression is the standard of care and sometimes modestly effective, there are currently no approved treatments for patients with CTD-associated ILD, highlighting the substantial need for large clinical trials, despite the significant challenges they may pose.
What Rheumatologists Need to Know
The summit underscored the recognition that practicing clinicians continue to struggle with in this arena because there are no good answers at this time. “Patients who have RA with ILD need better treatment for their ILD. Patients with scleroderma and ILD need better approaches to screening, management and therapy for their ILD. I look at this as a platform that’s been put forth with regards to unmet clinical and research needs and opportunities,” Dr. Fischer says.
A major takeaway from the summit was the emphasis to learn from idiopathic pulmonary fibrosis—both failures and successes with clinical trials, clinical trial design and implementation. “We have rare diseases,” Dr. Fischer says, “but with coordinated efforts, we can really put novel therapeutic agents into clinical trials and successfully recruit, enroll, design and foster clinical trials. So on a practical level, we hope to be able to see that the treatment paradigm for ILD is enriched by successfully conducted clinical trials.”
The summit was an indication of both the need for answers for patients with CTD-associated ILD as well as a high level of enthusiasm among clinicians and researchers who flew in from around the world in order to share information and collaborate.
“The enthusiasm for the effort leading up to this meeting and the work put in by the attendees, I think, speaks to an era of excitement and optimism that these kinds of efforts will lead to getting us the answers that we desperately need to help these patients,” Dr. Fischer says. “By getting different clinicians and researchers from across different specialties to interact and meet face to face, it really does foster future collaborative opportunities.”
Renée Bacher is a frequent contributor to ENT Today and the AARP Bulletin. Her article about heart disease in women, “This Story Could Save Your Life,” won a recent National Health Information Award for Family Circle magazine.
Reference
- Fischer A, Strek ME, Cottin V, et al. Proceedings of the American College of Rheumatology/Association of Physicians of Great Britain and Ireland Connective Tissue Disease-Associated Interstitial Lung Disease Summit: A multidisciplinary approach to address challenges and opportunities. Arthritis Rheumatol. 2019 Feb;71(2):182–195.