Targeted Therapeutics
In light of the recent advances in the understanding of the pathogenesis of SSc, new anti-fibrotic treatments are currently in development and being studied for the treatment of the disease (see Table 2). We will review some of these new treatments by their molecular targets.
(click for larger image)
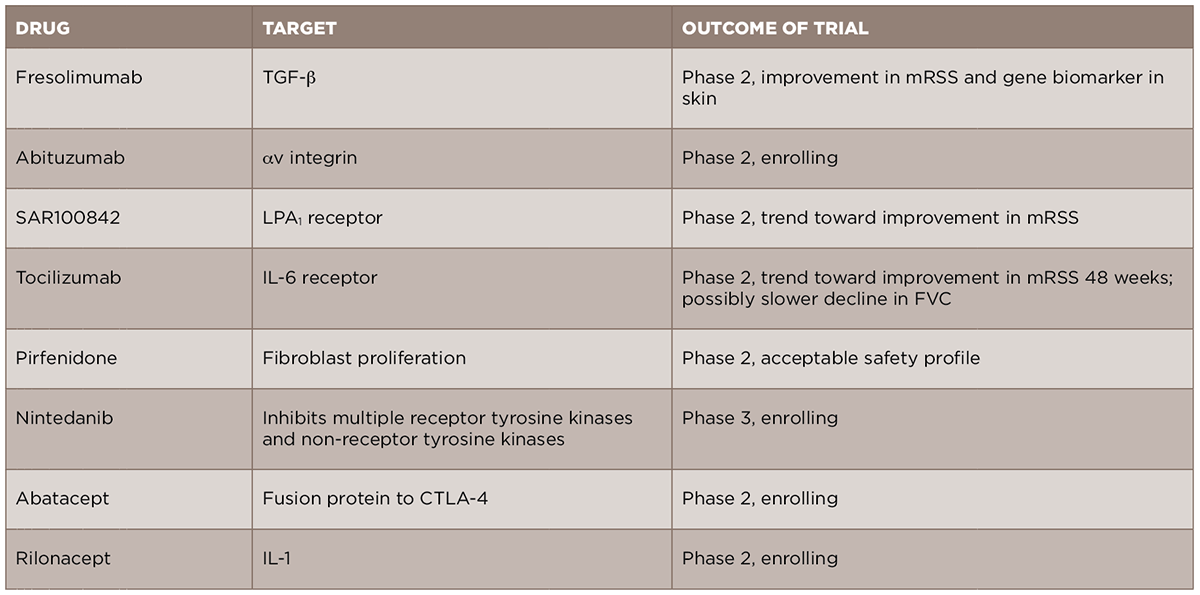
TABLE 2: New Targeted Therapeutics in Scleroderma Fibrosis
Given the central role of TGF-β in the development of scleroderma fibrosis, it is a natural target for therapy in SSc. A recent open-label trial of fresolimumab, a monoclonal antibody against TGF-β that neutralizes all isoforms of the molecule, compared two doses of the drug in patients with early (less than two years) dcSSc.17 The primary outcomes of this trial were change in mRSS and change in mRNA levels of two biomarkers measured in the skin, cartilage oligomeric protein (COMP) and thrombospondin-1 (THBS1), at 24 weeks. In both groups, there was a relatively rapid decrease in mRSS and in TGF-β regulated biomarker genes, in particular THBS1, suggesting that targeting TGF-β may be an effective treatment strategy. Of note, there were a number of cases of anemia in both groups, and this will need to be examined further in future, larger studies. Another drug targeting the TGF-β pathway, abituzumab, a monoclonal antibody against αv integrin, will be evaluated in an upcoming Phase 2 trial for SSc-ILD (ClinicalTrials.gov identifier: NCT02745145).
