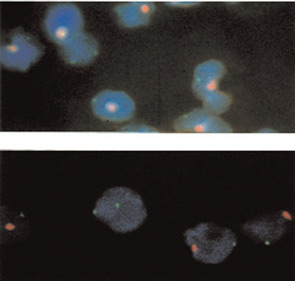
Figure 1: A female cell with two X chromosomes is seen among male cells with one Y and one X chromosome in peripheral blood from an adult male. The X chromosome is labeled with green and the Y chromosome with red fluorescent dye. (Fluorescence in situ hybridization of peripheral blood cells 100x.)
Source: J Clin Invest. 1999 Jul;104(1):41-47.
Source: J Clin Invest. 1999 Jul;104(1):41-47.
Microchimerism’s Role in Disease
The hypothesis that naturally acquired microchimerism is involved in some autoimmune disease was proposed after considering observations derived from different specialties of medicine.10 (See Figure 2) One observation was that an iatrogenic form of chimerism, graft-versus-host disease after hematopoietic cell transplantation, has many clinical similarities to autoimmune diseases—especially systemic sclerosis and also aspects of myositis and systemic lupus erythematosus.

