click for large version
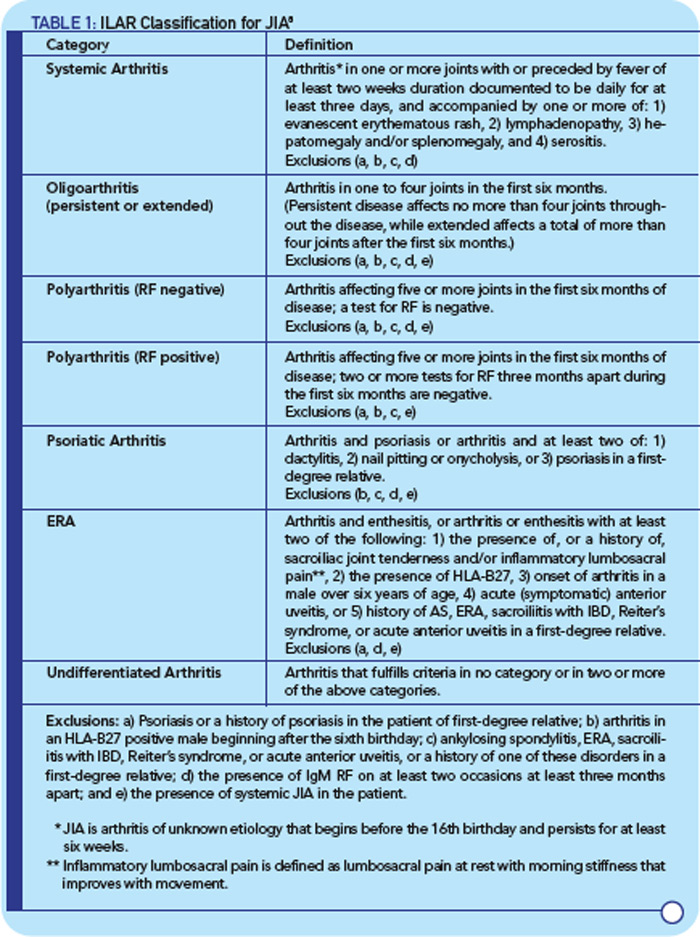
TABLE 1: ILAR Classification for JIA8
The Relationship Between Inflammation and Bone Formation
Important advances in the treatment of AS have been made in the last decade, largely as a result of the use of TNF-a inhibitors that improve symptoms and signs of disease, including pain and inflammation.17 However, there is evidence that TNF-a blockade does not prevent aberrant bone formation in the axial skeleton.18,19 This finding is consistent with results from a mouse model of SpA, where the incidence and severity of spontaneous joint ankylosis were unaffected by TNF-a inhibition.20 Other studies demonstrate that excess TNF-a actually inhibits bone formation through effects on both the Wnt and BMP pathways, as well as by promoting osteoclast development and activation.21,22


