
7Crafts / shutterstock.com
Many rheumatology patients have complex conditions and require the added expertise of colleagues in other fields, such as pulmonology, neurology or dermatology. This is even more true when patients with complex care issues are referred to academic medical centers. At such centers, patients often travel hours for an appointment and see more than one provider.
The University of Washington is the only academic medical center in the five-state region known as WWAMI (i.e., Washington, Wyoming, Alaska, Montana and Idaho), and it serves as a referral center for these states. Several years ago, we realized that if we wanted to better serve our patients’ needs, we should make it easy for them to see their physicians and get the care they need. We gradually started a series of combined clinics with willing colleagues. At these centers, rheumatologist(s) would attend clinics in which combined expertise was often needed, including dermatology/rheumatology, nephrology/rheumatology, neuromuscular/rheumatology and interstitial lung disease (ILD)/rheumatology clinics.
Combined clinics are not a new concept. Combined dermatology/rheumatology clinics are present at many academic institutions nationally and internationally, and many have focused on the combined treatment of psoriasis and psoriatic arthritis.1 Combining expertise has also led to the development of a fellowship at Brigham and Women’s Hospital in Boston in which a rheumatologist or dermatologist can pursue a one-year fellowship in the combined dermatology/rheumatology clinic. More than 20 academic institutions participate in a research consortium based on the combined dermatology/rheumatology model of the Psoriasis and Psoriatic Arthritis Clinics Multicenter Advancement Network (PPACMAN).2 In addition, combined clinics in other fields, such as ILD/rheumatology and myositis/rheumatology, operated for many years at the Cleveland Clinic, Louisiana State University, National Jewish Health in Denver, Johns Hopkins in Baltimore and other institutions.
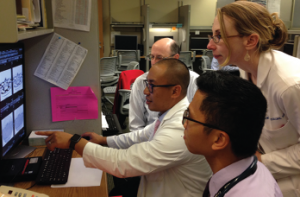
Dr. Lawrence Ho (pulmonary/ILD) points out important features of an HRCT scan to Dr. Greg Gardner (rheumatology), Dr. Percy Balderia (rheumatology fellow) and Dr. Bridget Collins (pulmonary ILD).
Clinics combine patient care in a variety of ways. Some simply schedule patients in different clinics on the same day, with interaction by phone or electronic medical record. Multidisciplinary conferences also provide combined care. Some combined clinics have specialists in the same clinic who see patients at different times, with a post-clinic conference or workroom interaction to discuss patient-care issues.

