Clinical Case
The clinical case follows a 29-year-old woman presenting with a six-month history of a pruritic rash that began after a viral illness. The patient’s symptoms include fatigue, hair loss and severe scalp pruritus. She was previously diagnosed with eczema, which did not improve on treatment with antihistamines and topical corticosteroids.
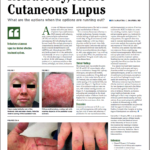
Clinical examination revealed violaceous periorbital edema, scaly red papules on the metacarpophalangeal joints of both hands, dilated capillaries of the proximal nail folds, scaly plaques on both elbows, and excoriated red plaques on her upper chest, back and hips. Antibody testing proved negative. The patient did not report any muscle weakness, strength and creatinine phosphokinase testing appeared normal, and magnetic resonance imaging of the thigh ruled out inflammation or edema.
The patient was diagnosed with clinically amyopathic dermatomyositis and treated with methotrexate, but this did not improve her skin and led to debilitating intractable pruritus. Mycophenolate mofetil treatment provided minimal improvement. However, given the lack of muscle involvement, the patient’s health insurance did not approve using intravenous immunoglobulin (IVIG).
The authors note that patients with clinically amyopathic dermatomyositis comprise up to 60% of dermatomyositis cases in dermatology clinics. As in the clinical case, “skin disease is often refractory to current systemic directed therapies and results in debilitating pruritus and increased morbidity,” the authors write. “Given the effectiveness of IVIG, and the likelihood of success with IVIG in this case, it is essential that dermatomyositis trials include amyopathic dermatomyositis patients so they can access appropriate therapies.”
Cutaneous Lupus Erythematosus vs. Dermatomyositis
Knowledge remains limited regarding both the pathogenesis of dermatomyositis and the drivers of skin disease.
The clinical case “raises several important issues related to the immunologic underpinnings of cutaneous lupus erythematosus and dermatomyositis,” including the roles of type I IFN in triggering skin disease and IFN in the pathogenesis of skin inflammation, the authors write. “Can we apply what we know about IFN-targeted therapeutics in cutaneous lupus erythematosus and dermatomyositis to develop better treatments for skin disease?”
Cutaneous lupus erythematosus and dermatomyositis remain challenging to differentiate, especially if the disease is limited to the skin, with rashes appearing similarly in both conditions. In dermatomyositis, as with cutaneous lupus erythematosus, type I IFNs appear highly upregulated in the blood, muscle and skin, correlating to disease activity. Further, in genetically predisposed individuals, cutaneous lupus erythematosus and dermatomyositis skin are likely induced or triggered by increased IFN exposure, as with sunlight, medications such as immune checkpoint inhibitors and hydroxyurea, immune-stimulating supplements or viral illnesses, including COVID-19.