When performing a RhUS examination, it’s critical to sweep the transducer across the entire target structure, or asymmetrically located pathologies (e.g., swollen synovium, effusion, erosion) may be missed.
Wrist
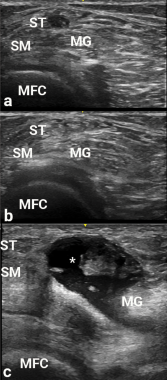
Figure 2
Images a, b and c are transverse
views of the medial popliteal space. Due to anisotropy, the semitendinosus area (adjacent to ST) is hypoechoic in appearance, and could be confused with a popliteal cyst. The ST become hyperechoic in b after transducer angle adjustment, thereby making the potential cyst disappear. In c, a real popliteal cyst (asterisk) is apparent between the semimembranosus (SM) and medial gastrocnemius (MG), and over the medial femoral condyle (MFC).
In obtaining the volar/palmar transverse view of the wrist, many found it challenging to visualize the median nerve without having the flexor tendons appear too dark due to anisotropy. Angling the probe/sound waves toward the elbow helps resolve this issue. This positioning requires a lot of nerve (sic, PD again).


