Ankle
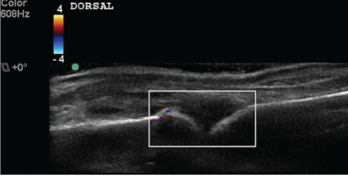
Figure 3
The Doppler View
Half of the participants stumbled in visualizing the posterior tibial tendon (PTT) insertion. The course of the PTT in the ankle and foot is as follows: around the posterior portion of the medial malleolus, then on the cranial surface of the sustentaculum tali, then inferior to the calcaneo-
navicular (i.e., spring) ligament. Finally, as it gets to the navicular, about half of its fibers attach to the navicular tuberosity (infero-medial surface of the navicular) and the medial cuneiform. Some recurrent fibers connect to the sustentaculum tali, and the remaining fibers continue to the plantar surface of the foot. Due to this unusual course, when imaging the PTT in its longitudinal view in the medial foot, the sound beam must be angled slightly cephalad to minimize anisotropy.4
A few fellows misidentified calcaneal erosion as osteophytes due to failure to correlate longitudinal with transverse images and construct a three-dimensional image of the Achilles insertion in their minds. Erosions are potholes in the bone, and osteophytes are jagged extrusions from the bone. These two will be confused only if the sonographer cannot determine where the normal bone surface is, and this mistake could lead to substantial diagnostic and treatment errors (see Figure 1). At this moment, the student tends to feel like a heel (sic, you know who).


