(Click for larger image)
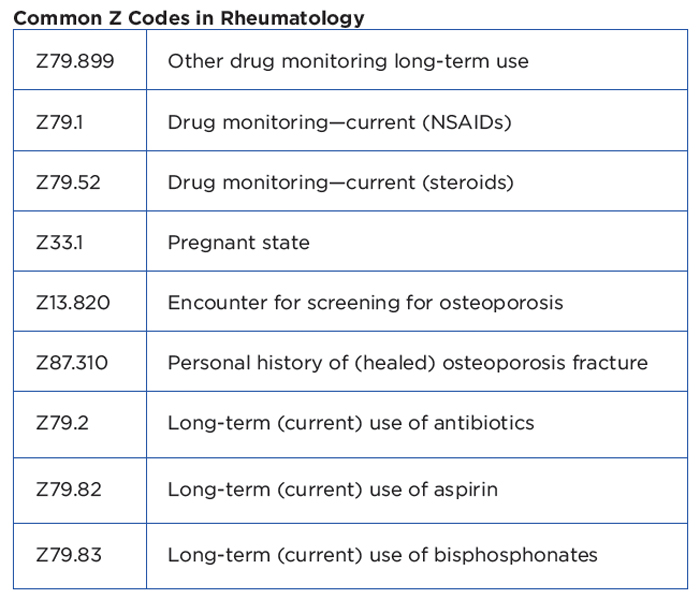
Common Z Codes in Rheumatology
It’s important to understand that status codes are informative; they have distinct categories for certain encounters and conditions. They can be reported in any health setting and may be used as a first-listed diagnosis (depending on the encounter or if for an inpatient setting) or secondary code, depending on the circumstances for the encounter. Status codes indicate that a patient is a carrier of a disease, has the sequelae or residual of a past disease or condition, or has another factor influencing their health status. Because status codes may affect the course of treatment and its outcome, the codes are used to track public health issues.
Are Z codes mandatory? The Official Coding Guidelines do not differentiate the use of Z codes from that of other codes (except W external codes). Z codes will most often be used to describe an encounter for testing or to identify a potential risk. In the case of using it as a principal diagnosis, this can be used mainly for osteoporosis. If there are no signs or symptoms of osteoporosis documented in a patient’s record, the screening code is correct. Although there are no specific coding rules for ICD-10 on this issue, the coding guidelines for ICD-10 are the same as ICD-9 (use screening: if there are no signs/symptoms, then the screening code should be used, but if there are signs/symptoms, then a specific diagnosis code should be applied). For example, if a postmenopausal patient undergoes a bone density study for screening for osteoporosis, Z13.820 (encounter for screening for osteoporosis) is recommended as the first code, and Z78.0 (asymptomatic menopausal state) as a secondary code.
