

Evidence Supporting Use of Bisphosphonates after Hip Fracture
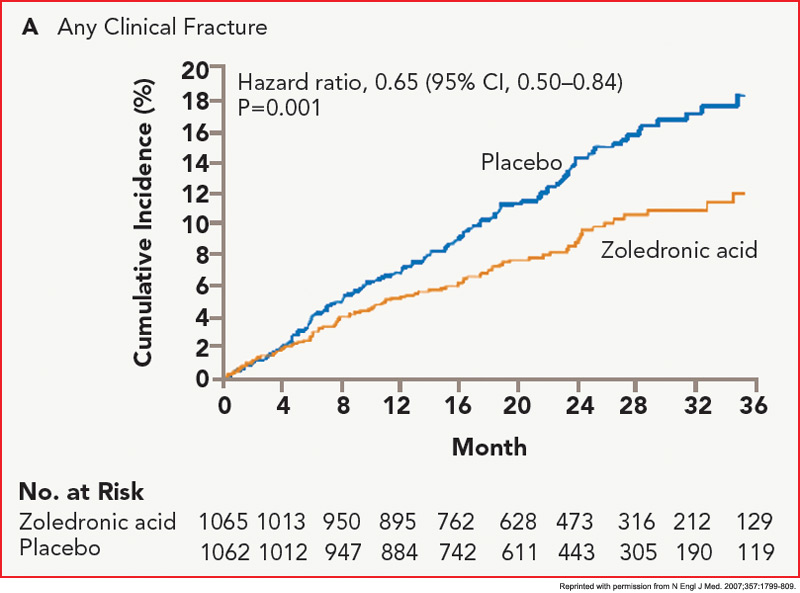
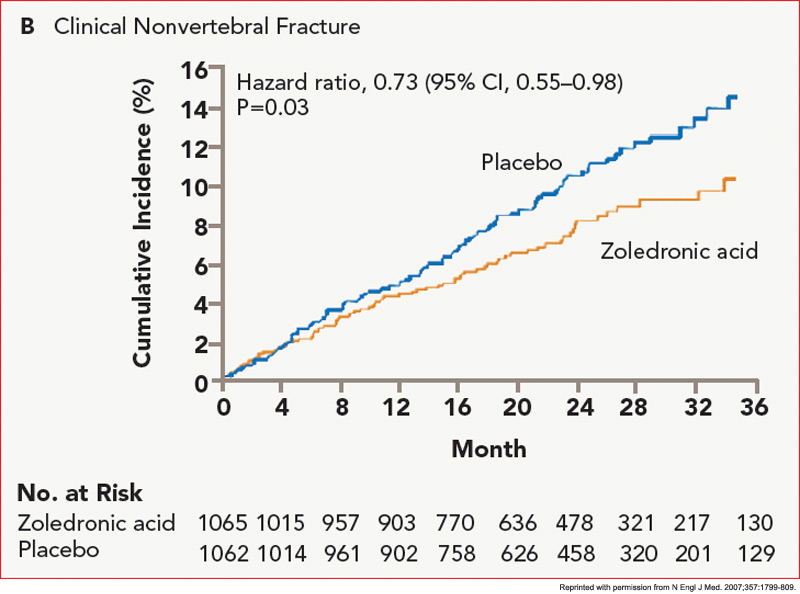
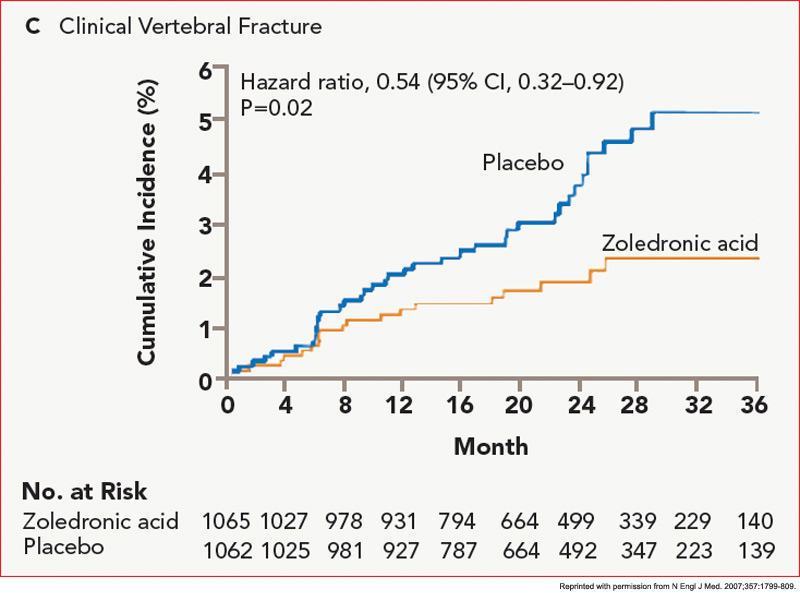
The HORIZON Recurrent Fracture Trial (HORIZON-RFT) was designed to determine the risks and benefits of bisphosphonate treatment in frail older adults with hip fracture. HORIZON-RFT was a randomized, controlled, double-blind study comparing zoledronic acid 5 mg IV yearly with a placebo. More than 2,100 patients were enrolled within 90 days of surgical repair of a low-trauma hip fracture, and were followed for up to three years for additional clinical fractures, bone mineral density (BMD), and safety endpoints including mortality (see Figure 1, above). Patients were enrolled from both community and institutional settings, but were ambulatory prior to the hip fracture. Other notable inclusion criteria were estimated GFR of greater than 30 mL/min, near-normal serum calcium levels, and inability or unwillingness to take an oral bisphosphonate. Because a large proportion of participants were found to be vitamin D insufficient, all participants received a loading dose of approximately 100,000 IU at least one week prior to the first dose of zoledronic acid, followed by daily oral calcium and vitamin D supplements. Patients were enrolled regardless of their baseline DXA, and 45% had T scores > –2.5.6


