arka38 / SHUTTERSTOCK.COM
SAN DIEGO—Recent research tells us more about giant cell arteritis (GCA) to help rheumatologists more accurately diagnose and effectively treat patients with this type of vasculitis. On Nov. 6 at the ACR/ARHP Annual Meeting, three experts explored the latest findings on GCA pathogenesis, diagnostic approaches, imaging modalities and growing treatment options.
GCA: What’s Really Happening?
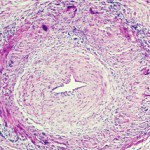
GCA is a granulomatous, large-vessel vasculitis that usually affects patients after 50, and women more often than men. GCA may affect the aorta and the smaller, second to fifth aortic branches, particularly the temporal artery, said Cornelia Weyand, MD, PhD, professor of medicine at Stanford University’s Vasculitis Research Center.