What really counts when coding is the basis of time. First, only face-to-face time with the patient and/or family member counts in the outpatient setting. Face-to-face time includes not only the time spent counseling, but also the time associated with any history, examination or MDM that is performed. Time spent reviewing records, talking with other providers and documenting the encounter without the patient or family present cannot be considered.
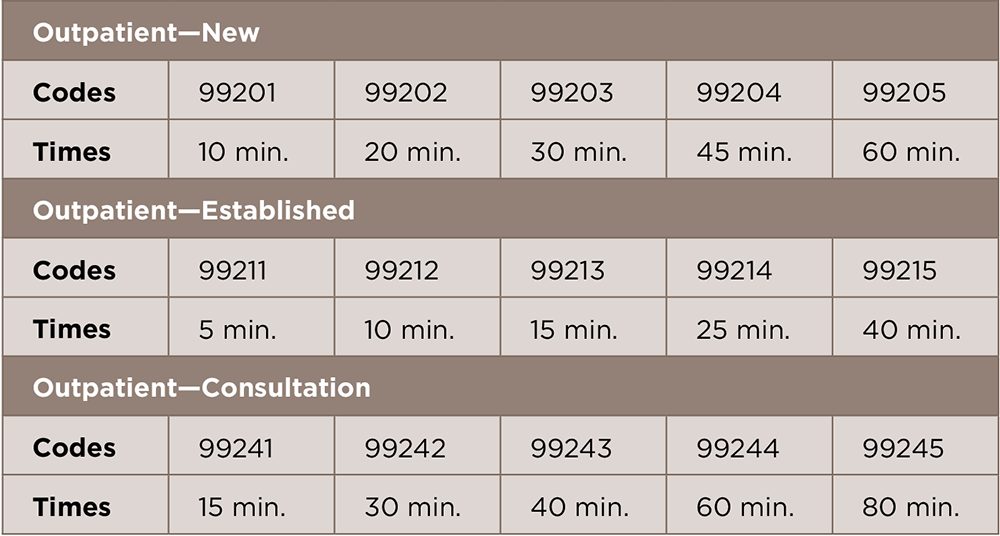
(click for larger image) TABLE 1: Typical Times for Outpatient E/M Services
Second, it is not enough to document only how long the service lasted or that counseling or coordination of care dominated the visit. The documentation must explain the content of the counseling discussion and must describe the activities to coordinate care to support time as the dominating factor, but most importantly, the medical necessity of the service.

