Evidence from a randomized trial has supported that MTX can be used to induce remission of nonsevere WG.9 Oral or subcutaneous MTX is started at 15 mg/week (0.3 mg/kg/week) and increased within the first two to four weeks to 20–25 mg/week. To reduce toxicity, MTX is given with folic acid 1 mg daily or folinic acid 5 mg once a week taken 24 hours after MTX.
click for large version
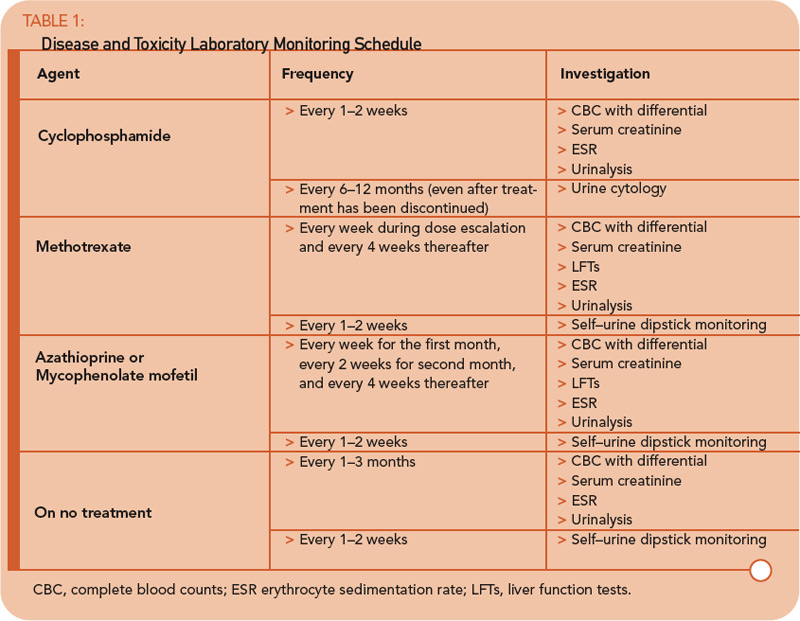
Table 1: Disease and Toxicity Laboratory Monitoring Schedule
Maintenance
To date, there have been no comparative trials among individual maintenance agents. Therefore, a decision about which medication to use must be based on individual factors, including contraindications and relapse history. In the absence of cytopenias, the maintenance agent can be started within one to two days after stopping CYC.