Gts/shutterstock.com
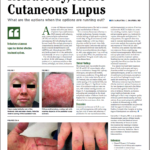
SAN FRANCISCO—A 40-year-old woman shows up in the clinic with scarring alopecia, with an area of hyperpigmentation on the rim of her scalp, extending from just behind the temple to behind her ears.
An examination with a dermatoscope shows hyperkeratotic follicular plugging.
The case—in this example, the discoid form of cutaneous lupus erythematosus (DLE)—is one slice of the wide array of skin issues that can arise in rheumatic diseases, which can present special challenges for the rheumatologist, an expert said in a clinical review session at the 2015 ACR/ARHP Annual Meeting.
Joseph Merola, MD, MMSc, assistant professor at Harvard Medical School, director of clinical trials and co-director of the Center for Skin and Related Musculoskeletal Diseases at Brigham and Women’s Hospital, said that a patient like this will have a key question: “What can you tell her about her risk of SLE?”
Cutaneous lupus (CLE) grouping schemes can be somewhat confusing, with CLE broadly grouped into types with specific lesions and non-specific lesions—what is known as the Modified Gilliam Grouping Schema. The so-called lupus specific lesion group is then sub-grouped into acute cutaneous LE, subacute LE and chronic cutaneous LE, which includes DLE.
There are limited data to answer the question of SLE risk, said Dr. Merola, who is dual-certified in dermatology and rheumatology. But cross-sectional prevalence data are available, he said. In DLE, localized lesions—those above the neck—are associated with SLE in around 5% of patients, while generalized lesions, about 20%. It seems that among those patients with DLE who are going to progress to SLE, the majority do so within five years of DLE diagnosis. Unpublished data at Dr. Merola’s center suggest this might happen much sooner than five years out, he said.
Subacute cutaneous LE (SCLE) is associated with SLE about 50% of the time; acute CLE, including malar eruption, about 90%. Lupus panniculitis is associated with SLE about 10% of the time, while tumid CLE, a rare variant of the chronic cutaneous form, essentially never does, Dr. Merola said.
Despite earlier reports, it appears that SLE patients with DLE are at a lower risk of arthritis and serositis than SLE patients without DLE, but have about the same risk of nephritis and end-stage renal disease.1
Subacute Cutaneous Lupus Erythematosus (SCLE)
There is an ever-increasing number of medications associated with drug-induced SCLE. A frequent question that arises when patients present with SCLE is whether it is idiopathic or drug induced. Dr. Merola presented an example of a patient who was started on adalimumab for seropositive, erosive rheumatoid arthritis two months earlier, and had a biopsy that was “consistent with connective tissue disease including cutaneous lupus.” She was also positive for anti-SSA/Ro antibodies.