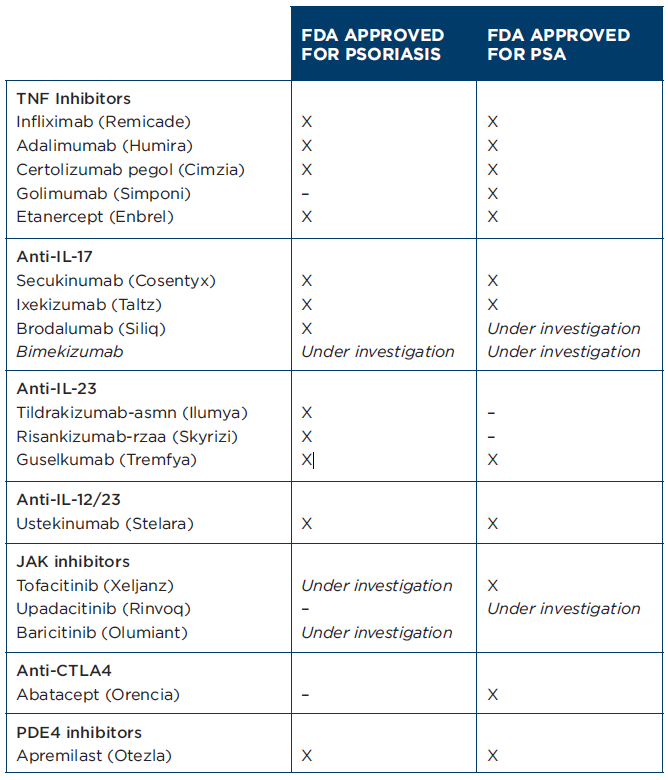
Figure 1: Biologic DMARDS FDA-approved for psoriasis and PsA as of August 2021. (Click to enlarge.)
“There is a still a role for methotrexate in the management of psoriasis, but it is getting smaller,” says Dr. Evans. “Methotrexate can still be used as an inexpensive first-line agent in certain situations. It is also often used as an adjunct agent to biologics to improve efficacy and possibly inhibit anti-drug antibodies. My perception is that dermatologists use it less often than other specialists, and that use continues to decrease as more biologic and oral options become available.”
In terms of when he reaches for a biologic to treat psoriasis, Dr. Evans says, “Biologics are commonly firstline agents in the modern treatment of psoriasis, especially severe psoriasis that either covers a large body surface area, or affects sensitive sites like the hands, feet, genitals or scalp. They can also be added when topicals, ultraviolet B, and oral agents have failed. It is generally more based on patient specific factors than an inflexible algorithm.”



