click for large version
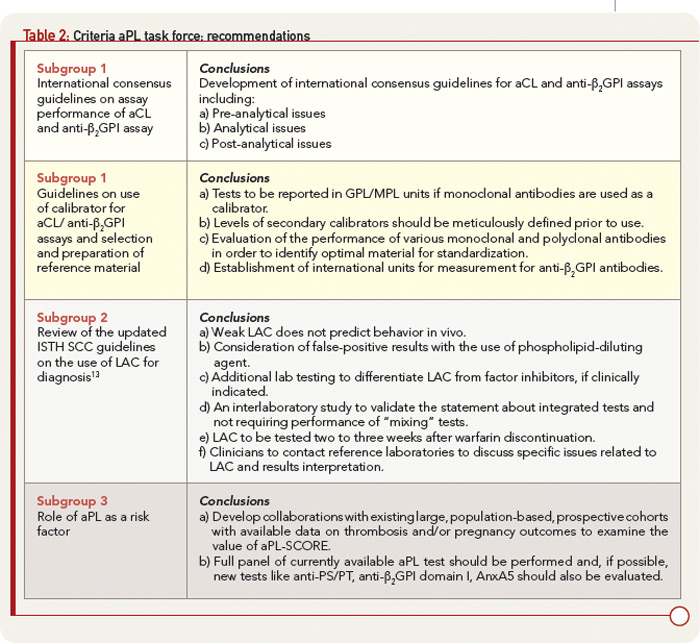
Table 2: Criteria aPL task force: recommendations
Subgroup 3
The group evaluated the possibility of using results of aPL antibody tests to calculate “risk factors” for APS-related clinical manifestations. Otomo and colleagues have described an antiphospholipid score (aPL-S), a weighted summation of results from LAC, aCL, anti-β2GPI, and anti–phosphatidylserine/prothrombin (anti–PS/PT) assays based on odds ratios. A higher prevalence of APS clinical manifestations was observed in patients with higher aPL-S, suggesting the use of a cluster analysis in the future to predict an APS risk factor. Also, when considering groups of tests, the risk of APS was found to be calculated as higher if the data were analyzed by cluster analysis or by combining the results of more than one test (aCL, anti-β2GPI, LAC).
