Technology as a Tool for Safety Research
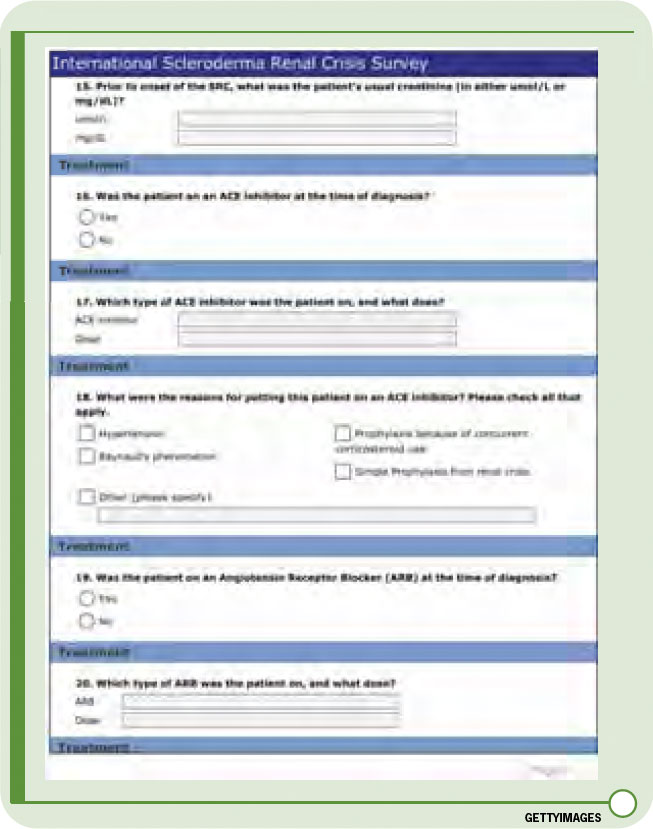
Our question was, Could the Internet help us perform this study? Many of us have probably already participated in studies using the Internet. Who has not received a set of questions on SurveyMonkey or a similar questionnaire program? John “Jack” Cush, MD, of Baylor Research Institute in Dallas, has performed several surveys using the ACR’s e-mail list, and he has used Internet technology to study various issues such as rheumatologists’ impressions of the use of musculoskeletal ultrasound. Many of us have also participated in Delphi exercises to obtain experts consensus opinions. However, my colleague Marie Hudson, MD, a rheumatologist at the Jewish General Hospital and assistant professor of Medicine at McGill University, both in Montreal, realized that the Internet could be used as a unique resource for the study of SRC, a rare complication of an uncommon disease.