A salt-and-pepper appearance of the skin is … one of the earliest cutaneous findings in systemic sclerosis.
Discussion
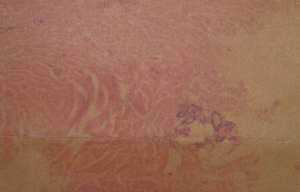
Figure 5. A skin biopsy revealed superficial and deep dermal perivascular lymphocytic infiltrate and focally increased dermal collageny.
Systemic sclerosis is a heterogeneous disorder characterized by dysfunction of the endothelium, dysregulation of fibroblasts (resulting in excessive production of collagen) and immune system abnormalities.7 Although the cause of SSc remains unknown, genetic and environmental factors are believed to contribute to host susceptibility.8 SSc is divided into diffuse cutaneous and limited cutaneous syndromes, depending on the extent of skin thickening. These classically manifest as Raynaud’s phenomenon, sclerodactyly, esophageal dysmotility and a range of organ-specific complications.1 Systemic involvement may occur in the form of pulmonary vasculopathy, interstitial fibrosis, cardiomyopathy, arrhythmia, conduction abnormality, acute renal crisis, etc.2

