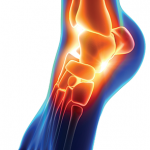
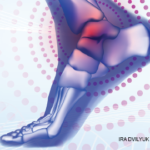
Figure 1: Salient Features of the Patient Exam
The top left panel shows synovitis in the right second through fourth metacarpal phalangeal joints, with large subcutaneous cysts involving the distal forearm and wrist. The top right panel shows a right forearm lesion with overlying ulceration. The bottom left panel demonstrates marked swelling in left ankle. The bottom right panel shows scattered ulcerations on the upper left arm.
A 61-year-old Caucasian woman with a history of seropositive rheumatoid arthritis (RA) was hospitalized for a several-month history of progressively worsening left ankle pain and swelling.
She had been unable to bear weight on her left leg for several days and did not notice improvement in symptoms with 20 mg of prednisone daily, which she had increased to 40 mg daily a few days prior to admission. Her right wrist and hand were also painful and swollen. Over the preceding months, she had noted progressively enlarging, painful nodules on her right forearm, one of which had spontaneously drained yellow-tinged fluid. She had also developed ulcerations over some of the nodules and the contralateral forearm. She did not have any preceding trauma to the right upper extremity. A review of systems was notable for several months of intermittent night sweats.