Syphilis has been historically referred to as the great mimicker given its heterogenous presentation.3,4 The three stages of infection are: primary, secondary and tertiary. Our patient likely had secondary infection, with rash and lymphadenopathy. Renal involvement can occur at any stage, from secondary to latent and tertiary. Both SLE and syphilis can have multi-system involvement.
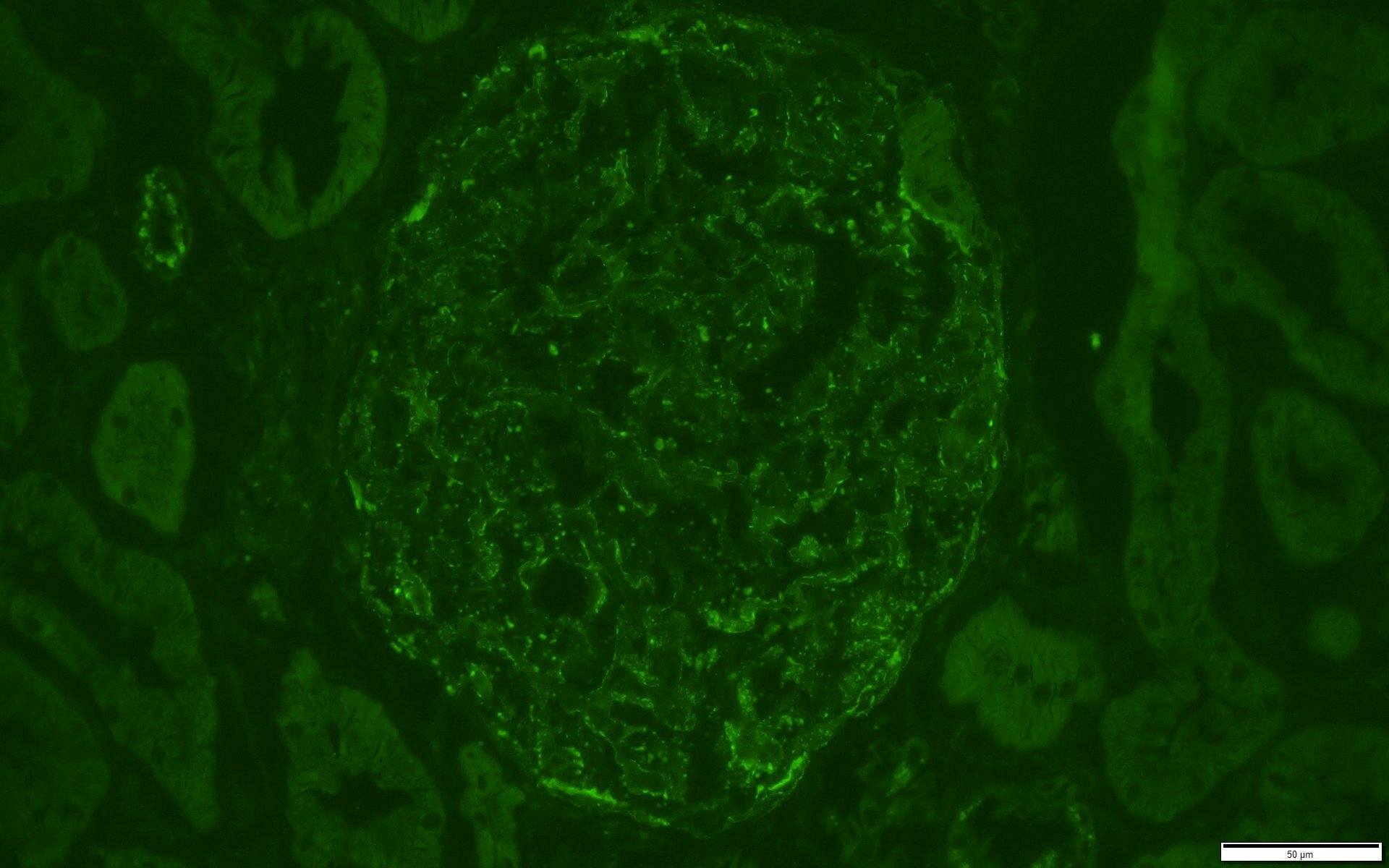
FIGURE 4: IMMUNOFLUORESCENCE C1Q STAIN
Trace staining also noted for C1q in similar distribution as IgG stain.
[mobile-ad name="Advert 2"](Click to enlarge.)
This case illustrates the importance of thinking about infectious etiologies for glomerulonephritis and completing a thorough sexual history. Further, the diagnosis of lupus nephritis should be questioned when serologic and other laboratory markers (e.g., anti-Smith and double-stranded DNA antibodies, low complement levels, cytopenias) and clinical manifestations of lupus are absent, despite suggestive renal histology findings. The presence of C1q is nearly pathognomonic for lupus nephritis, but can also be seen when parvovirus B19 causes kidney disease.1 Parvovirus B19 and syphilis have been reported to cause the same histologic features of lupus nephritis. 1,3,4-6
In Sum
It’s important to recognize the above etiologies of membranous nephropathy because the correct diagnosis has treatment implications. The nephrotic syndrome associated with parvovirus B19 infection may improve spontaneously and that with syphilis improves with penicillin.3,5-7 A similar case of co-infection with both parvovirus B19 and syphilis improved with antibiotic treatment for syphilis.1
Matthew J. Mandell, DO, is a staff rheumatologist at Cleveland Clinic. He completed his rheumatology fellowship training at the University of Iowa Hospitals & Clinics, Iowa City.
Yishui Chen, MD, is a second-year neurology resident at the University of Iowa Hospitals & Clinics.