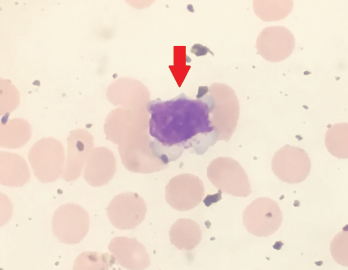
Figure 1. Peripheral blood smear showing a large granular lymphocyte in a 53-year-old Hispanic man.
Large granular lymphocytic (LGL) leukemia is a rare, chronic, lymphoproliferative disorder of cytotoxic T cell or natural killer cell lineage with an annual incidence of 0.72 cases per 1 million people in the U.S.1 The most common subtype of LGL leukemia, T-LGL leukemia, follows an indolent disease course and accounts for approximately 85% of cases. A second subtype, the chronic, lymphoproliferative disorder of natural killer cells (CLPD-NK), accounts for less than 10% of cases. The third subtype, known as aggressive natural killer-LGL leukemia, accounts for less than 5% of cases and carries a poor prognosis because it is refractory to chemotherapy.2,3
The diagnosis is made by first identifying an increased population of circulating large granular lymphocytic cells. An absolute lymphocyte count of >2,000 lymphocytes/mL may be helpful; however, it’s not mandatory because the diagnosis can be made if a clonal large granular lymphocytic population is identified in the clinical setting of autoimmune disease, such as rheumatoid arthritis or cytopenias (e.g., neutropenia, anemia, thrombocytopenia).2,4
