
Valentyn Volkov / shutterstock.com
Idiopathic inflammatory myopathies are heterogenous, acquired immune-mediated muscle diseases. Over the past decade, immune-mediated necrotizing myopathy has been recognized as a subcategory of idiopathic inflammatory myopathy characterized by myofiber necrosis in the absence of prominent inflammatory cells.1 Autoantibodies against signal recognition particle (SRP) and 3-hydroxy-3-methylglutaryl-coenzyme A reductase (HMGCR) are thought to be associated with the development of immune-mediated necrotizing myopathy. The latter was originally identified in patients exposed to statin in the U.S. and was initially thought to be specific to statin-associated necrotizing myopathy.2 In East Asia, however, the rate of statin-naive immune-mediated necrotizing myopathy seems to be much higher than in North America.3-5
In this article, we present a case of statin-naive, anti-HMGCR and anti-SRP antibody-positive immune-mediated necrotizing myopathy possibly associated with the daily ingestion of shiitake mushrooms (Lentinula edodes).
A physical examination showed his vital signs were within normal limits. Auscultation of lungs and heart was normal. He had muscle tenderness over his back and both thighs. Manual muscle testing revealed mild weakness only in the hip flexors (4/5 on the medical research council scale), but he had normal strength in the rest of his muscles.
On laboratory tests (see Table 1), his serum CK level was 1,280 IU/L. Anti-nuclear antibody immunofluorescence staining showed cytoplasmic pattern (1:80). Anti-Jo-1 and other selected autoantibodies were negative.
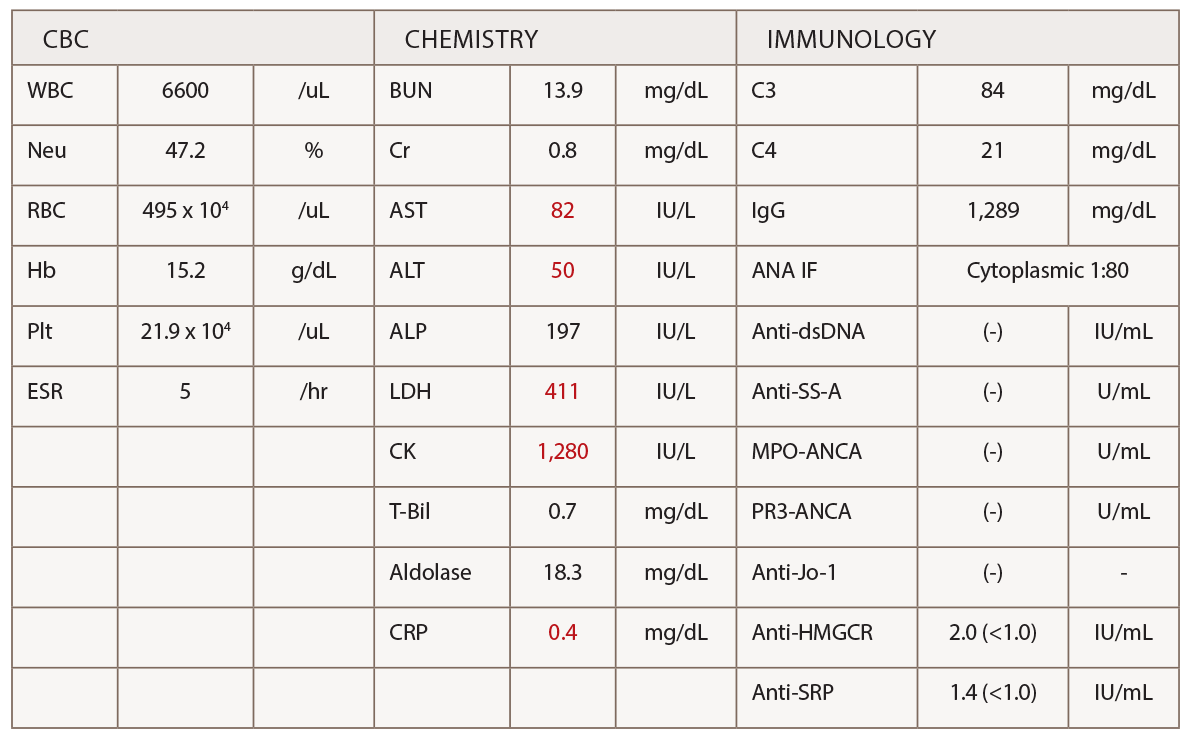
(click for larger image) Table 1: Laboratory Tests
Abbreviations: ANA IF; antinuclear antibody immunofluorescence staining, Anti-dsDNA; anti-double strand DNA antibody, MPO-ANCA; myeloperoxidase anti-neutrophil cytoplasmic antibody, PR3-ANCA; proteinase-3 anti-neutrophil cytoplasmic antibody.
A magnetic resonance imaging scan of his arms and legs did not reveal any abnormalities. A needle electromyography did not show signs of irritable myopathy.
Despite these unremarkable test results, we suspected immune-mediated necrotizing myopathy based on otherwise unexplainable myalgia and CK elevation, as well as the history of daily consumption of shiitake mushrooms. We performed muscle biopsy of the left biceps brachii and obtained blood for further analysis for autoantibodies associated with idiopathic inflammatory myopathies.
The muscle biopsy (see Figure 1) showed one necrotic and several internally nucleated fibers, in addition to moderate upregulation of MHC class I staining, raising a possibility of immune-mediated necrotizing myopathy—albeit complement C5b-9 was not deposited on the sarcolemma. The autoantibody analyses using enzyme-linked immunosorbent assay (ELISA) revealed both anti-HMGCR and anti-SRP antibodies were positive (antibody titer 2.0 IU/mL and 1.4 IU/mL, respectively; cutoff 1.0 IU/mL).


