Tupungato; Svetlana Voronova/shutterstock.com
The levels of service within an evaluation and management (E/M) visit are based on the documentation of key components, which include history, physical examination and medical decision making. The history component is comparable to telling a story and should include a beginning and some form of development to adequately describe the patient’s presenting problem.
To ensure high-quality patient care and proper reimbursement, it is important that documentation of the history element tell the complete story of why the patient is in the office. The Centers for Medicare and Medicaid Services (CMS) Documentation Guidelines for Evaluation and Management Services have four history levels, each of which comprises four elements.1 To qualify for a given history level, certain elements are required, as depicted in Table 1.
Note from the table that as the type of history becomes more intensive, the elements required to perform that type of history also increase in intensity. For example, a problem-focused history requires documentation of the chief complaint (CC) and a brief history of present illness (HPI), while a detailed history requires the documentation of a CC, an extended HPI, plus an extended review of systems (ROS) and pertinent past, family and/or social history (PFSH).
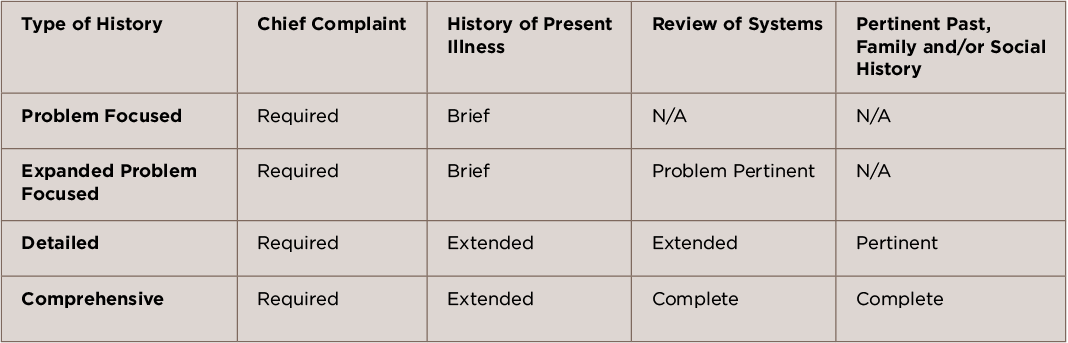
(click for larger image) TABLE 1
Elements of History
Each type of history includes some or all of the following elements: CC, HPI, ROS and PFSH.
