In this review article, we describe the diagnostic criteria (including the clinical and histological features) for immunoglobin G4-related kidney disease (IgG4-RKD), including the renal and other organ manifestations in IgG4-RKD, the pathophysiology and treatment.
Diagnostic Criteria
The diagnostic algorithm for IgG4-RKD includes the presence of kidney injury, as manifested by abnormal urinalysis or urine markers, abnormal radiologic findings or decreased kidney function with characteristic serological findings.6
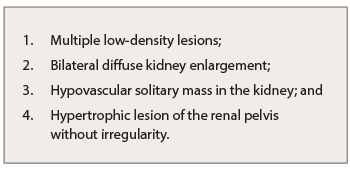
Table 1: Abnormal Renal Radiologic Findings of IgG4-RKD
Abnormal renal radiologic findings are usually the first distinctive elements of this rare entity (see Table 1). Of these, the most common radiologic features include multiple low-density lesions on enhanced computed tomography (CT). Bilateral diffuse kidney enlargement can appear in plain CT. In addition, radiology might detect a (rare) hypovascular solitary mass in the kidney—in that case, malignancy must be ruled out. The fourth radiologic abnormality includes hypertrophic lesion of the renal pelvis without irregularity of the renal pelvic surface. Urinary tract carcinoma is considered the most important condition in the differential diagnosis.7
Kidney injury is recognized by the presence of proteinuria, hematuria and elevated N-acetyl-β-D-glucosaminidase, β2-microglobulin and/or α1-microglobulin excretions in urinalysis (UA). Hypergammaglobulinemia or elevated serum IgG levels (>135 mg/dL), low complement and elevated serum IgE levels are all frequent serologic findings of IgG4-RKD, and at least one of these three abnormalities is necessary for the diagnosis (see Table 2 ).2,7