Kateryna Kon / shutterstock.com
CHICAGO—At the 2018 ACR/ARHP Annual Meeting, Allen C. Steere, MD, delivered the Rheumatology Research Foundation Memorial Lecture honoring the late Charles M. Plotz, MD: Linking Gut Microbial Immunity with Autoimmunity in Joints in Patients with Rheumatoid Arthritis. Dr. Steere is professor of medicine at Harvard Medical School, Boston, and director of translational research in rheumatology at Massachusetts General Hospital. His ongoing research focuses on the possible role of infectious agents in the microbiome, particularly Prevatella copri, in the initiation and perpetuation of pathogenic immune responses in rheumatoid arthritis (RA).
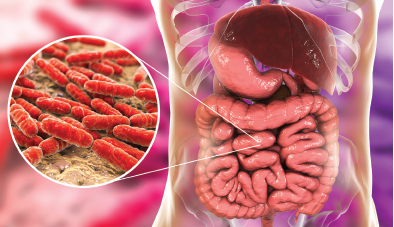
Bacterial Colonies in the Gut
Rheumatologists have made great progress in understanding RA’s genetic risk factors, but are only now identifying its environmental factors, said Dr. Steere. His lecture focused on the gut as a potential site of immune stimulation.