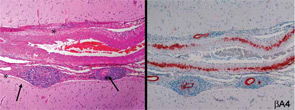
Figure 1: Histopathologic features of open brain biopsy from a patient with primary central nervous system vasculitis showing presence of a granulomatous pattern with amyloid angiopathy. The left panel shows destructive vasculitis with well-formed granulomas involving the leptomeningeal vessels (arrows) and wall thickening with eosinophilic material (asterisk) (hematoxylin and eosin × 100). The right panel shows Aβ deposits in all vessels (immunoperoxidase staining for βA4 amyloid ×100).
Because of the clinical history and MRI findings, a diagnosis of primary central nervous system vasculitis (PCNSV) was considered, and an open brain biopsy was performed. Pathology showed granulomatous leptomeningeal and intraparenchymal vasculitis. Infarcts and vascular beta-A4 amyloid deposition consistent with cerebral amyloid angiopathy (CAA) were also present (see Figure 1). Stains of biopsy specimens were negative for fungal and mycobacterial organisms.