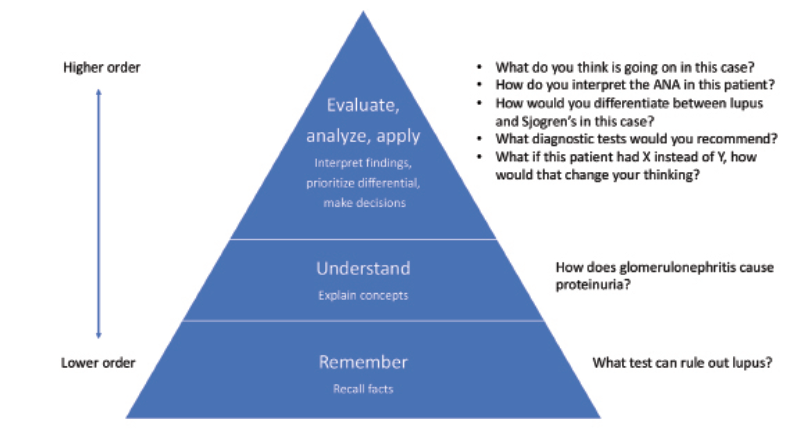
Table 3: Adapted Bloom’s Taxonomy & Question Phrasing
After the Encounter
The post-encounter period is an important time to extend the educational opportunities provided by the patient evaluation. Shared experience and direct observation of learners allow the preceptor to provide more specific feedback, which ideally highlights what the learner should continue to do as well as areas for improvement.10,11 The latter can then serve as focus points for continued learning in the post-encounter period, either by providing a resource to review or asking the learner to look something up that can be revisited at a future time.
Including the learner in post-encounter communications with other members of the care team requires little additional time, but we have found it can make the learner feel like a valued part of the team while also exposing them to multidisciplinary care.

