The Prediction Rule
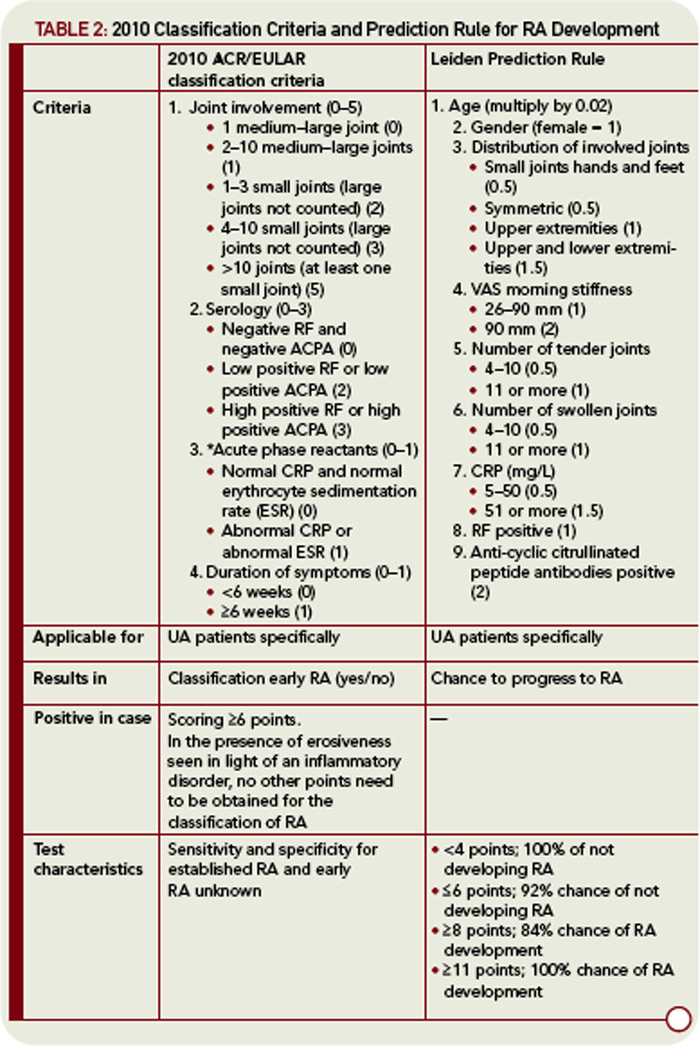
Given the intricacy and difficulty of deriving totally independent criteria for early RA, another option to identify early RA patients is to develop a predictive tool. For this purpose, the current classification criteria do not need to be changed. A prediction tool of this kind has recently been developed.7 This tool consists of nine variables: age, gender, distribution of involved joints, severity of morning stiffness, number of tender joints, number of swollen joints, C-reactive protein (CRP), RF, and anti-cyclic citrullinated peptide antibodies (see Table 2, p. 24). Intriguingly, these variables are quite similar to those in the 2010 ACR/EULAR criteria and contain elements of arthritis indicating joint pathology, inflammation, and autoantibodies. This prediction rule has been derived from prospective data and did not rely on expert opinion for its development. Although this rule was developed based on the experience of a single early arthritis cohort, it has an adequate discriminative ability and the predictive ability of this model has been validated in multiple worldwide studies.8–13
