The prophylactic use of pentoxifylline & tocopherol two to three weeks prior to a dental extraction & continued therapy post extraction until the surgical site completely heals have been shown to reduce the incidence of MRONJ.
Autologous Platelet Concentrates
In 1998, Marx et al. reported the use of platelet-rich fibrin (PRF) as an accelerator in bone healing by influencing bone regeneration. PRF is obtained by sequestering and concentrating platelets by gradient density centrifugation.15 It is an autogenous source of platelet-derived growth factors, transforming growth factor β1 and transforming growth factor β2.15 Hence, PRF is responsible for enhancing the rate of wound healing and new bone formation. Since 1998, autologous platelet concentrates have gained popularity in oral and maxillofacial surgery. Its advantages and beneficial effects for improved soft tissue and bone healing have been validated in several other oral surgery procedures, as well.
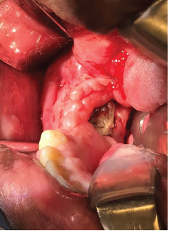
Exposed bone in the right mandible.
In 2007, Adornato et al. reported their experience using platelet-derived growth factors in managing refractory cases of MRONJ in 12 patients. They treated patients with a combination of the removal of necrotic bone and the application of PRF with resorbable collagen membrane.16 This therapy showed positive results, including complete wound healing, reduced treatment periods, less pain and improved quality of life.16
In 2012, Bocanegra-Perez et al. carried out a prospective descriptive study that included eight patients with a diagnosis of MRONJ. These patients were treated surgically with debridement of necrotic bone, followed by the application of leukocytes and PRF, and primary closure of the surgical site. The patients remained asymptomatic without dehiscence and evidence of exposed bone after an average 14-month follow-up period.17


